

Natural history, trajectory, and management of mechanically ventilated COVID-19 patients in the United Kingdom
- PMID: 33974106
- PMCID: PMC8111053
- DOI: 10.1007/s00134-021-06389-z
Natural history, trajectory, and management of mechanically ventilated COVID-19 patients in the United Kingdom
Abstract
Purpose: The trajectory of mechanically ventilated patients with coronavirus disease 2019 (COVID-19) is essential for clinical decisions, yet the focus so far has been on admission characteristics without consideration of the dynamic course of the disease in the context of applied therapeutic interventions.
Methods: We included adult patients undergoing invasive mechanical ventilation (IMV) within 48 h of intensive care unit (ICU) admission with complete clinical data until ICU death or discharge. We examined the importance of factors associated with disease progression over the first week, implementation and responsiveness to interventions used in acute respiratory distress syndrome (ARDS), and ICU outcome. We used machine learning (ML) and Explainable Artificial Intelligence (XAI) methods to characterise the evolution of clinical parameters and our ICU data visualisation tool is available as a web-based widget ( https://www.CovidUK.ICU ).
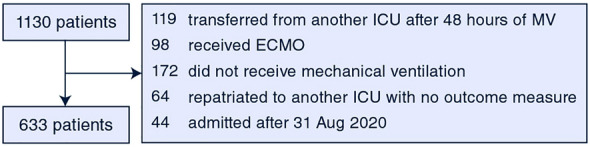
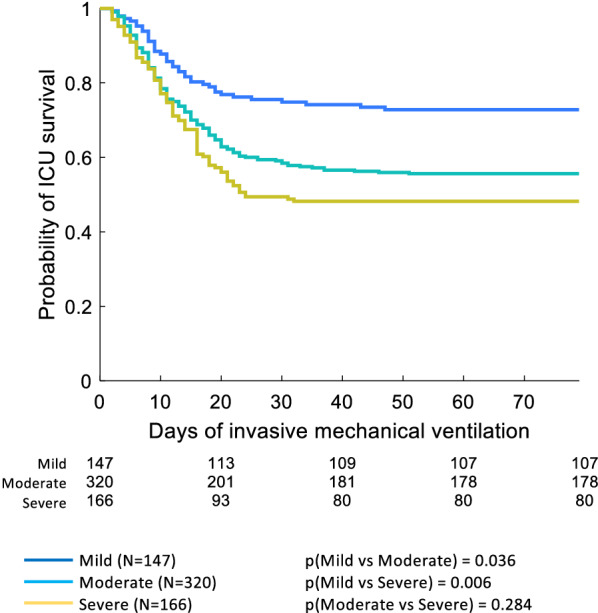
Results: Data for 633 adults with COVID-19 who underwent IMV between 01 March 2020 and 31 August 2020 were analysed. Overall mortality was 43.3% and highest with non-resolution of hypoxaemia [60.4% vs17.6%; P < 0.001; median PaO2/FiO2 on the day of death was 12.3(8.9-18.4) kPa] and non-response to proning (69.5% vs.31.1%; P < 0.001). Two ML models using weeklong data demonstrated an increased predictive accuracy for mortality compared to admission data (74.5% and 76.3% vs 60%, respectively). XAI models highlighted the increasing importance, over the first week, of PaO2/FiO2 in predicting mortality. Prone positioning improved oxygenation only in 45% of patients. A higher peak pressure (OR 1.42[1.06-1.91]; P < 0.05), raised respiratory component (OR 1.71[ 1.17-2.5]; P < 0.01) and cardiovascular component (OR 1.36 [1.04-1.75]; P < 0.05) of the sequential organ failure assessment (SOFA) score and raised lactate (OR 1.33 [0.99-1.79]; P = 0.057) immediately prior to application of prone positioning were associated with lack of oxygenation response. Prone positioning was not applied to 76% of patients with moderate hypoxemia and 45% of those with severe hypoxemia and patients who died without receiving proning interventions had more missed opportunities for prone intervention [7 (3-15.5) versus 2 (0-6); P < 0.001]. Despite the severity of gas exchange deficit, most patients received lung-protective ventilation with tidal volumes less than 8 mL/kg and plateau pressures less than 30cmH2O. This was despite systematic errors in measurement of height and derived ideal body weight.
Conclusions: Refractory hypoxaemia remains a major association with mortality, yet evidence based ARDS interventions, in particular prone positioning, were not implemented and had delayed application with an associated reduced responsiveness. Real-time service evaluation techniques offer opportunities to assess the delivery of care and improve protocolised implementation of evidence-based ARDS interventions, which might be associated with improvements in survival.
Keywords: ARDS; Artificial intelligence; COVID-19; Mechanical ventilation; Mortality risk; Prone position.
Conflict of interest statement
BVP reports consulting fees from GSK and Faraday Health; grants from Mermaid Care A/C, grants from ESICM, grants from Royal Brompton & Harefield Charity, grants from European Commission, grants from Academy of Medical Sciences, grants from Imperial College London Covid Fund. ACG reports grants from NIHR Imperial BRC, grants from NIHR Research Professorship, during the conduct of the study; other from Bristol-Meyers Squibb, other from GSK. ZP reports honoraria for consultancy from GlaxoSmithKline, Lyric Pharmaceuticals, Faraday Pharmaceuticals and Fresenius-Kabi, and speaker fees from Orion, Baxter, Nutricia and Nestle and educational grants from Baxter and VitaFlo. AAF reports grants from Imperial College London and the UKRI, during the conduct of the study. All other authors report no conflicts of interest.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
