

African Americans With p16+ and p16- Oropharyngeal Squamous Cell Carcinomas Have Distinctly Poor Treatment Outcomes Independent of Medical Care Access
- PMID: 33974822
- PMCID: PMC8257878
- DOI: 10.1200/OP.20.01105
African Americans With p16+ and p16- Oropharyngeal Squamous Cell Carcinomas Have Distinctly Poor Treatment Outcomes Independent of Medical Care Access
Abstract
Purpose: Human papilloma virus-positive (HPV+) oropharyngeal squamous cell carcinoma (OPSCC), diagnosed with p16 immunohistochemistry, is associated with favorable prognosis; however, this connection was established using European American (EA)-skewed populations. The impact of p16/human papillomavirus status on outcomes in African American (AA) OPSCC patients remains to be settled. In this study, we determine the association between cancer disparity and p16 status in an OPSCC cohort controlling for time to treatment initiation (TTI), a surrogate for medical care access.
Materials and methods: We analyzed data from all patients diagnosed with OPSCC (N = 440) between 2010 and 2017, who received treatment at our academic medical center. Associations between age, disease stage, sex, p16 status, race, TTI, and overall survival (OS) were investigated.
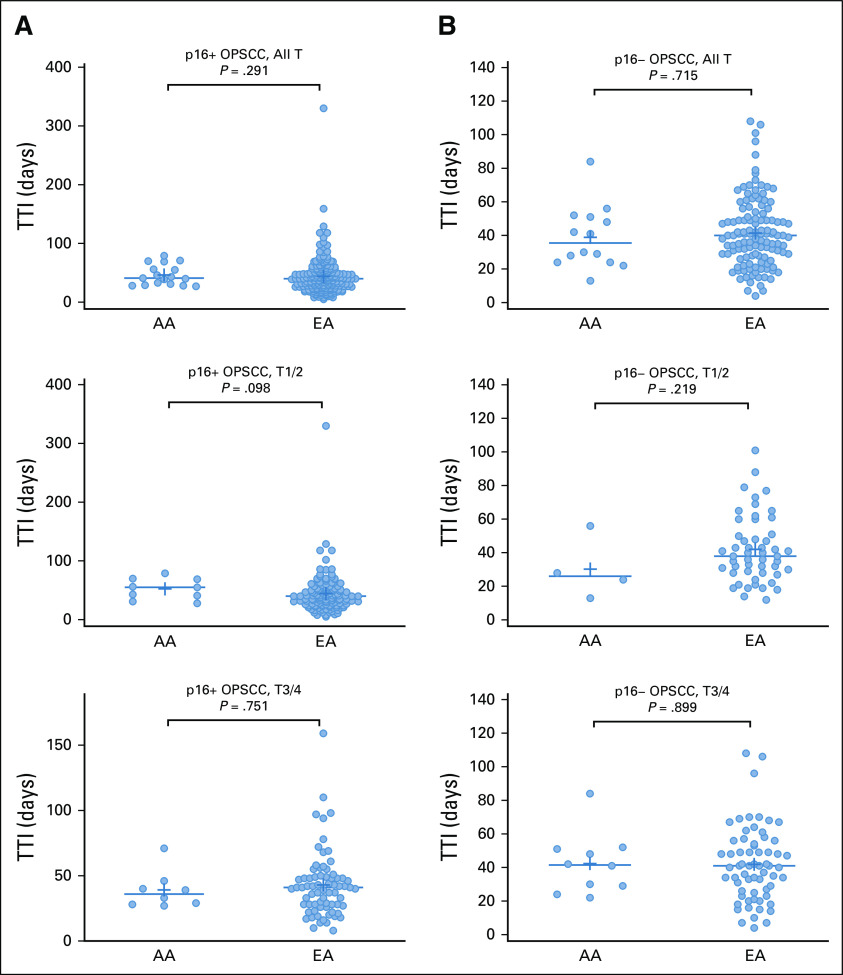
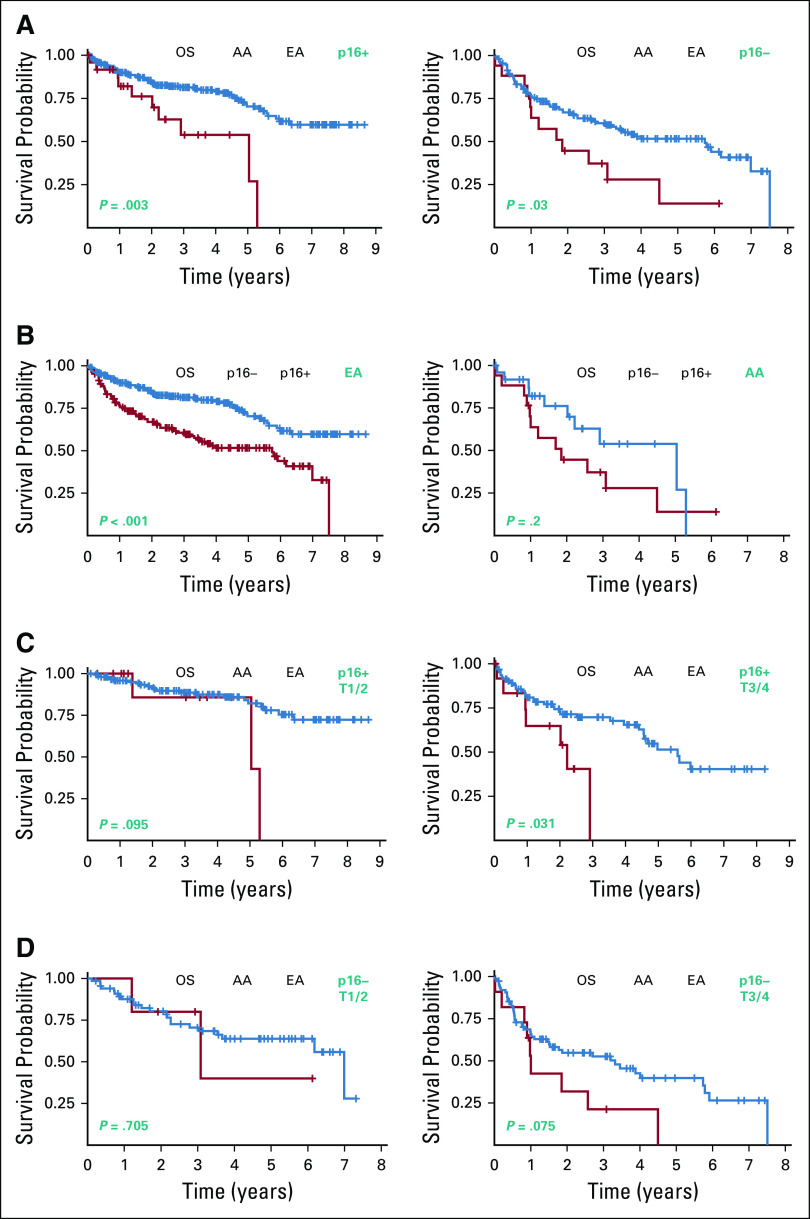
Results: TTI was similar between AA and EA OPSCC patients in our p16+ (P = .291) or p16- (P = .715) cohorts. Among p16+ OPSCC patients, the median OS was > 8.65 years for EA patients compared with 5.038 years (95% CI, 2.019 to 5.30; P = .003, log-rank) for AA patients. For p16- patients, the median OS was 5.74 years (95% CI, 3.32 to 6.99) for EA patients and 1.85 years (95% CI, 0.978 to 4.50; P = .03, log-rank) for AA patients. Multivariate Cox regression analysis showed that race was an independent prognostic biomarker and the most impactful co-variate for OS (hazard ratio, 0.40; 95% CI, 0.00 to 0.69; P = .001).
Conclusion: Our work showed that AAs with p16+ OPSCC have surprisingly poor clinical outcomes and are thus poor candidates for treatment de-escalation regimens. Caution should be exercised when extending clinical guidelines based on EA-majority studies to non-EA populations.
Conflict of interest statement
Figures
References
-
- Chlebowski RT, Chen Z, Anderson GL, et al. : Ethnicity and breast cancer: Factors influencing differences in incidence and outcome. J Natl Cancer Inst 97:439-448, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
