

The Optimal Age to Stop Endoscopic Surveillance of Patients With Barrett's Esophagus Based on Sex and Comorbidity: A Comparative Cost-Effectiveness Analysis
- PMID: 33974935
- PMCID: PMC8495224
- DOI: 10.1053/j.gastro.2021.05.003
The Optimal Age to Stop Endoscopic Surveillance of Patients With Barrett's Esophagus Based on Sex and Comorbidity: A Comparative Cost-Effectiveness Analysis
Abstract
Background and aims: Current guidelines recommend surveillance for patients with nondysplastic Barrett's esophagus (NDBE) but do not include a recommended age for discontinuing surveillance. This study aimed to determine the optimal age for last surveillance of NDBE patients stratified by sex and level of comorbidity.
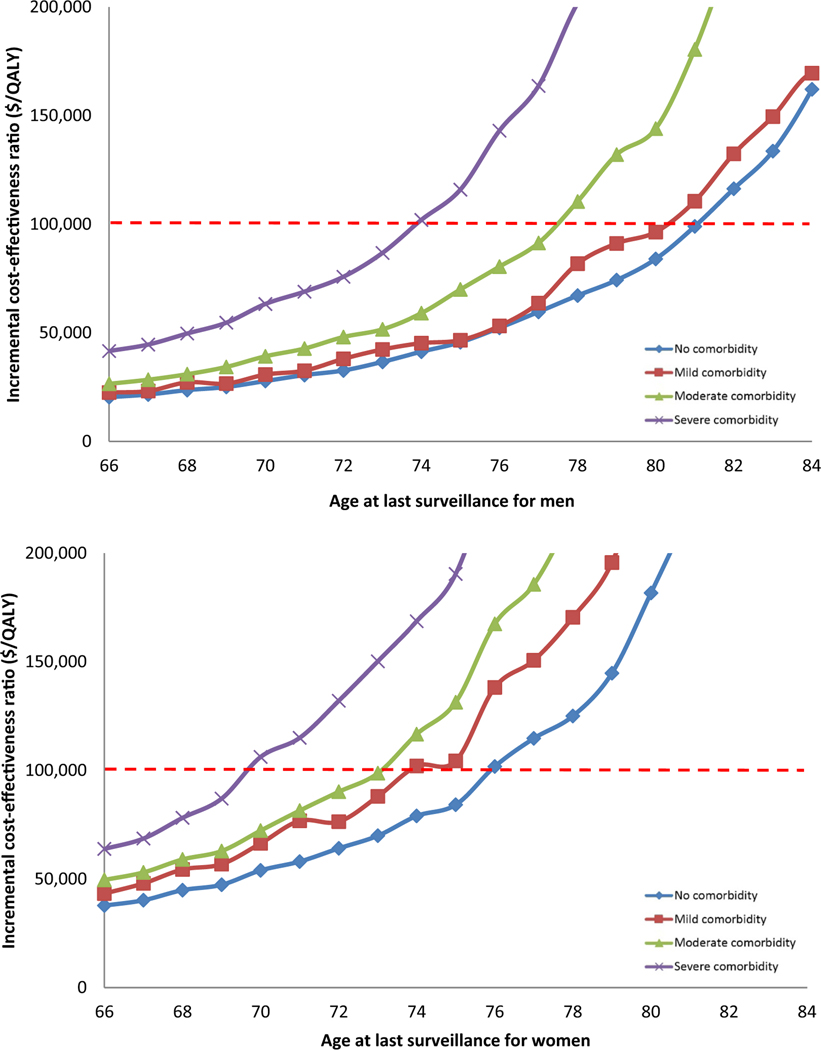
Methods: We used 3 independently developed models to simulate patients diagnosed with NDBE, varying in age, sex, and comorbidity level (no, mild, moderate, and severe). All patients had received regular surveillance until their current age. We calculated incremental costs and quality-adjusted life-years (QALYs) gained from 1 additional endoscopic surveillance at the current age versus not performing surveillance at that age. We determined the optimal age to end surveillance as the age at which incremental cost-effectiveness ratio of 1 more surveillance was just less than the willingness-to-pay threshold of $100,000/QALY.
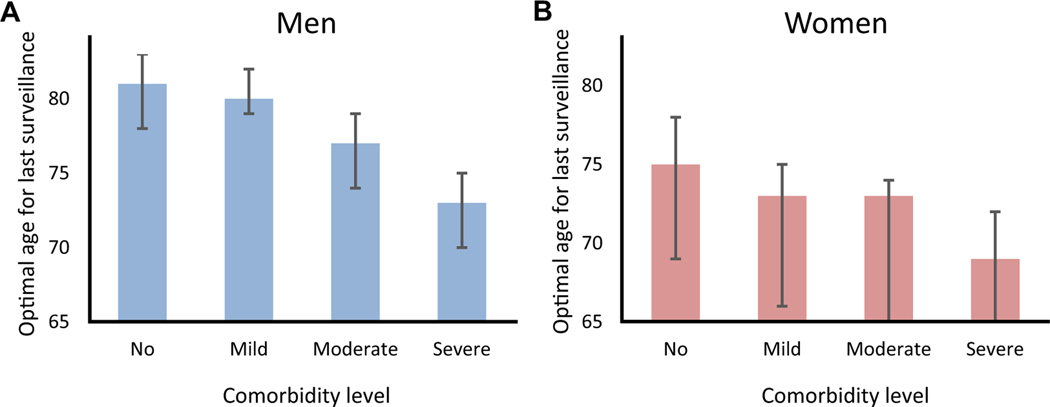
Results: The benefit of having 1 more surveillance endoscopy strongly depended on age, sex, and comorbidity. For men with NDBE and severe comorbidity, 1 additional surveillance at age 80 years provided 4 more QALYs per 1000 patients with BE at an additional cost of $1.2 million, whereas for women with severe comorbidity the benefit at that age was 7 QALYs at a cost of $1.3 million. For men with no, mild, moderate, and severe comorbidity, the optimal ages of last surveillance were 81, 80, 77, and 73 years, respectively. For women, these ages were younger: 75, 73, 73, and 69 years, respectively.
Conclusions: Our comparative modeling analysis illustrates the importance of considering comorbidity status and sex when deciding on the age to discontinue surveillance in patients with NDBE.
Keywords: CEA; EAC; Esophageal Cancer; Stop Age.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Varying Costs of Endoscopic Surveillance May Affect the Follow-Up Endpoint Identified by Cost-Benefit Analysis in Barrett's Esophagus Patients Around the World.Gastroenterology. 2022 Jan;162(1):351. doi: 10.1053/j.gastro.2021.06.010. Epub 2021 Jun 11. Gastroenterology. 2022. PMID: 34126064 No abstract available.
-
Reply.Gastroenterology. 2022 Jan;162(1):351-352. doi: 10.1053/j.gastro.2021.09.056. Epub 2021 Sep 28. Gastroenterology. 2022. PMID: 34597673 No abstract available.
References
-
- Rustgi AK, El-Serag HB. Esophageal carcinoma. N Engl J Med 2014;371:2499–2509. - PubMed
-
- Thrift AP. Barrett’s esophagus and esophageal adenocarcinoma: how common are they really? Dig Dis Sci 2018;63:1988–1996. - PubMed
-
- Standards of Practice Committee, C, Wani S, Qumseya B, et al. Endoscopic eradication therapy for patients with Barrett’s esophagus-associated dysplasia and intramucosal cancer. Gastrointest Endosc 2018; 87:907–931.e9. - PubMed
-
- American Gastroenterological Association, Spechler SJ, Sharma P, et al. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology 2011;140:1084–1091. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
