

Robotic open-thoracotomy-view approach using vertical port placement and confronting monitor setting
- PMID: 33975347
- PMCID: PMC8759507
- DOI: 10.1093/icvts/ivab033
Robotic open-thoracotomy-view approach using vertical port placement and confronting monitor setting
Abstract
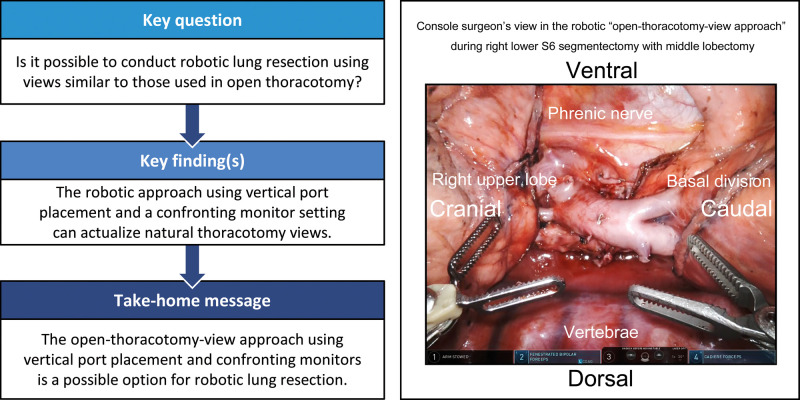
Objectives: Robotic lung resections (RLRs) are conventionally performed using look-up views of the thorax from the caudal side. To conduct RLR with views similar to those in open thoracotomy, we adopted a vertical port placement and confronting upside-down monitor setting, which we called robotic 'open-thoracotomy-view approach'. We herein present our experience of this procedure.
Methods: We retrospectively reviewed 58 patients who underwent RLR (43 with lobectomy; 15 with segmentectomy) with 3-arm open-thoracotomy-view approach using the da Vinci Surgical System between February 2019 and October 2020. The patient cart was rolled in from the left cranial side of the patient regardless of the side to be operated on. Robotic ports were vertically placed along the axillary line, and 2 confronting monitors and 2 assistants were positioned on each side of the patient. The right-side monitor, which was set up for the left-side assistant to view, projected the upside-down image of the console surgeon's view.
Results: All procedures were safely performed. The median duration of surgery and console operation was 215 and 164 min, respectively. Emergency conversion into thoracotomy and severe morbidities did not occur, and the median postoperative hospitalization duration was 3 days. In all procedures, the console surgeon and 2 assistants had direct 'bird-eye' views of the cranially located intrathoracic structures and instrument tips, which are sometimes undetectable with the conventional look-up view.
Conclusions: The open-thoracotomy-view approach setting is a possible option for RLR. It offers natural thoracotomy views and can circumvent some of the known limitations of the conventional procedure.
Keywords: Confronting monitors; Open-thoracotomy-view approach; Robotic lung resection; Vertical port placement.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures




References
-
- Cerfolio RJ, Watson C, Minnich DJ, Calloway S, Wei B.. One hundred planned robotic segmentectomies: early results, technical details, and preferred port placement. Ann Thorac Surg 2016;101:1089–95. - PubMed
-
- Jiao W, Zhao Y, Qiu T, Xuan Y, Sun X, Qin Y. et al. Robotic bronchial sleeve lobectomy for central lung tumors: technique and outcome. Ann Thorac Surg 2019;108:211–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
