

Efficacy and tolerability of atypical antipsychotics for acute bipolar depression: a network meta-analysis
- PMID: 33975574
- PMCID: PMC8112003
- DOI: 10.1186/s12888-021-03220-3
Efficacy and tolerability of atypical antipsychotics for acute bipolar depression: a network meta-analysis
Abstract
Background: While clinical trial evidence has firmly established the efficacy of several atypical antipsychotics (AAPs) for treating bipolar depression, no randomized controlled trials (RCT's) comparing AAPs have been conducted. This Bayesian network meta-analysis (NMA) compared the relative efficacy and tolerability of AAP monotherapy in adults with bipolar depression.
Methods: Efficacy measures included change in Montgomery Åsberg Depression Rating Scale (MADRS), Clinical Global Improvement - Bipolar Disorder (CGI-BP), response, and remission. Multiple tolerability outcomes were examined. Results from random effects models were reported as difference in change from baseline for continuous variables or odds ratios for dichotomous variables. Treatments were ranked using the surface under the curve cumulative ranking probabilities. Number needed to treat (NNT) and harm (NNH) were calculated.
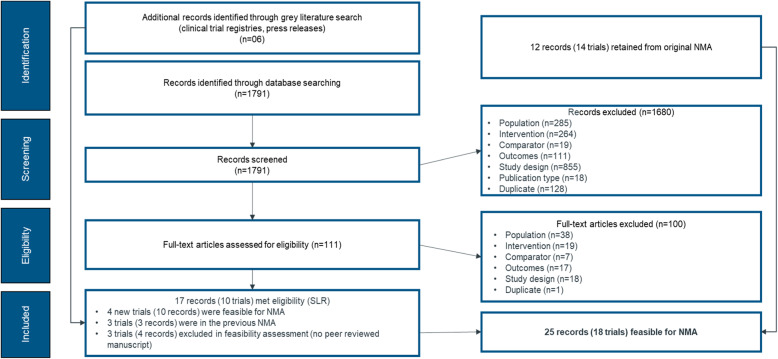
Results: Eighteen RCT's met inclusion criteria of the systematic literature review. On change in MADRS, lurasidone (- 4.71 [95% Crl - 6.98, - 2.41]), quetiapine (- 4.80 [- 5.93, - 3.72]), olanzapine (- 4.57 [- 5.92, - 3.20]), and cariprazine (- 2.29 [- 3.47, - 1.09]) were more efficacious than placebo. Lurasidone was associated with a significantly greater odds of response (≥50% improvement in MADRS) compared to cariprazine (1.78 [95% Crl 1.08, 2.77]), aripiprazole (2.38 [1.38, 3.85]), and ziprasidone (2.47 [1.41, 3.98]), but was similar to olanzapine (1.68 [0.99,2.65]) and quetiapine (1.25 [0.78, 1.90]). For change in CGI-BP-S-overall score, lurasidone was significantly better than cariprazine (- 0.38 [95% Crl - 0.66,-0.10]) and ziprasidone (- 0.58 [- 0.91,-0.26]), but similar to quetiapine (- 0.08 [- 0.36, 0.19])and olanzapine (- 0.04 [- 1.41, 1.46]). Lurasidone (0.34 kg [95% Crl - 0.22, 0.89]) and aripiprazole (0.20 kg [- 0.59, 1.00]) had a similar weight change compared to placebo, but olanzapine (2.88 kg [2.40, 3.36]), quetiapine (1.17 kg [0.84, 1.49]), and cariprazine (0.65 kg [0.34, 0.96]) were associated with greater weight gain. The NNT for response was the lowest for lurasidone (NNT = 5) followed by quetiapine (NNT = 6), olanzapine (NNT = 10) and cariprazine (NNT = 12).
Conclusions: In this NMA in adults with bipolar depression, which evaluated change in depressive symptoms (assessed by MADRS) across short-term trials, the largest improvement versus placebo was observed for lurasidone, olanzapine and quetiapine with cariprazine, showing a smaller treatment effect. Aripiprazole and ziprasidone were ineffective for the treatment of bipolar depression. Improvement in CGI-BP-S score for lurasidone was larger than cariprazine and ziprasidone but similar to quetiapine and olanzapine. Based on short term studies lurasidone and aripiprazole had similar weight gain compared to placebo.
Conflict of interest statement
Aditi Kadakia, Carole Dembek, and Antony Loebel are all full-time employees of Sunovion Pharmaceuticals Inc. the sponsor of the study and manufacturer of lurasidone (brand name Latuda). Sunovion Pharmaceuticals Inc. is a wholly owned subsidiary of Sumitomo Dainippon Pharma Co. Katsuhiko Hagi and Tadashi Nosaka are full time employees of Sumitomo Dainippon Pharma Co. Remaining Authors have no competing interest.
References
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders: DSM-5. 5. Washington, D.C: American Psychiatric Association; 2013.
-
- Merikangas KR, Jin R, He JP, Kessler RC, Lee S, Sampson NA, Viana MC, Andrade LH, Hu C, Karam EG, Ladea M, Medina-Mora ME, Ono Y, Posada-Villa J, Sagar R, Wells JE, Zarkov Z. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251. doi: 10.1001/archgenpsychiatry.2011.12. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
