

Prospective Case-Control Study of Cardiovascular Abnormalities 6 Months Following Mild COVID-19 in Healthcare Workers
- PMID: 33975819
- PMCID: PMC8105493
- DOI: 10.1016/j.jcmg.2021.04.011
Prospective Case-Control Study of Cardiovascular Abnormalities 6 Months Following Mild COVID-19 in Healthcare Workers
Abstract
Objectives: The purpose of this study was to detect cardiovascular changes after mild severe acute respiratory syndrome-coronavirus-2 infection.
Background: Concern exists that mild coronavirus disease 2019 may cause myocardial and vascular disease.
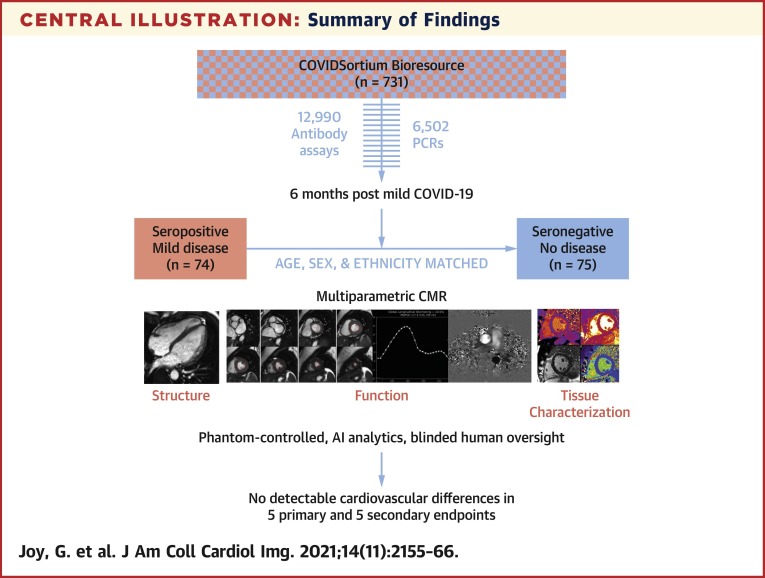
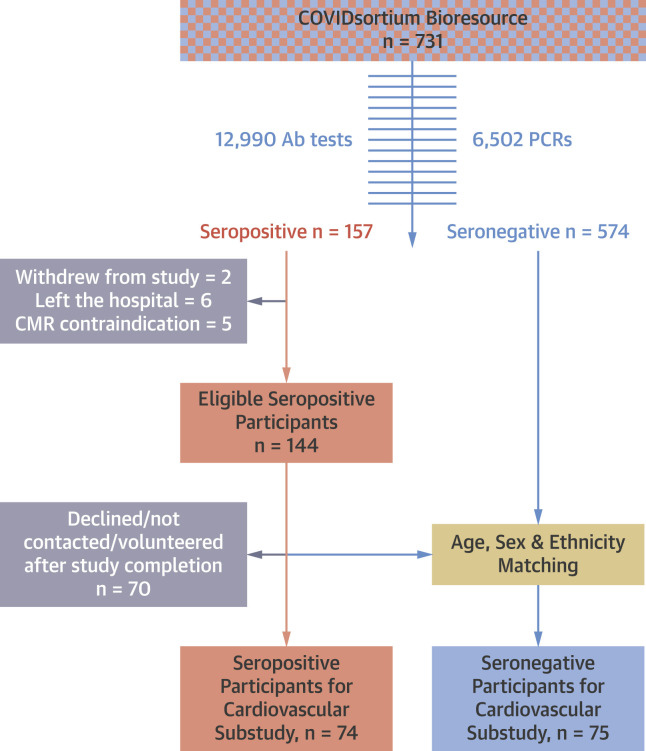
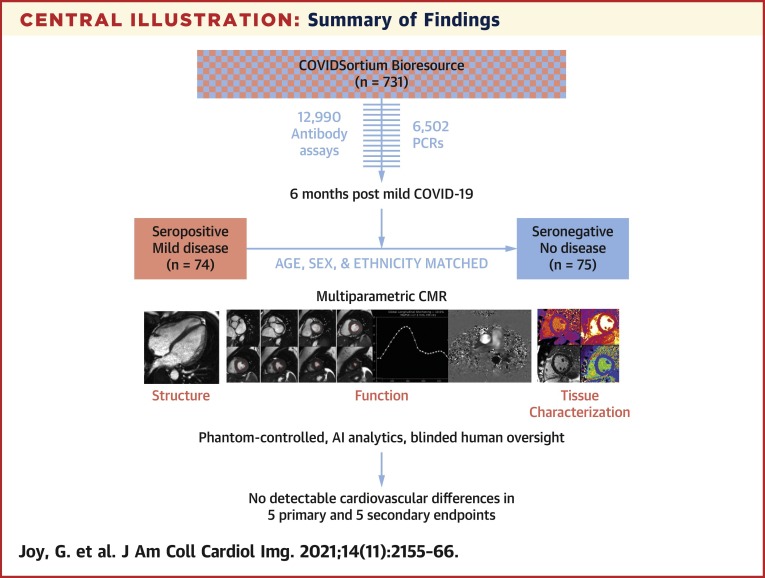
Methods: Participants were recruited from COVIDsortium, a 3-hospital prospective study of 731 health care workers who underwent first-wave weekly symptom, polymerase chain reaction, and serology assessment over 4 months, with seroconversion in 21.5% (n = 157). At 6 months post-infection, 74 seropositive and 75 age-, sex-, and ethnicity-matched seronegative control subjects were recruited for cardiovascular phenotyping (comprehensive phantom-calibrated cardiovascular magnetic resonance and blood biomarkers). Analysis was blinded, using objective artificial intelligence analytics where available.
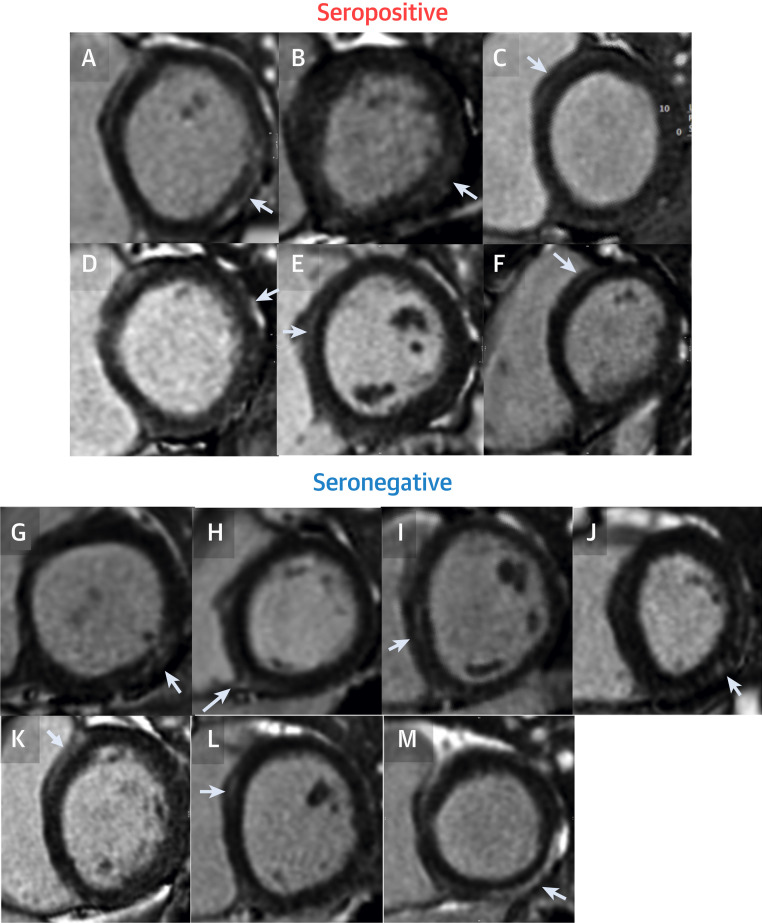
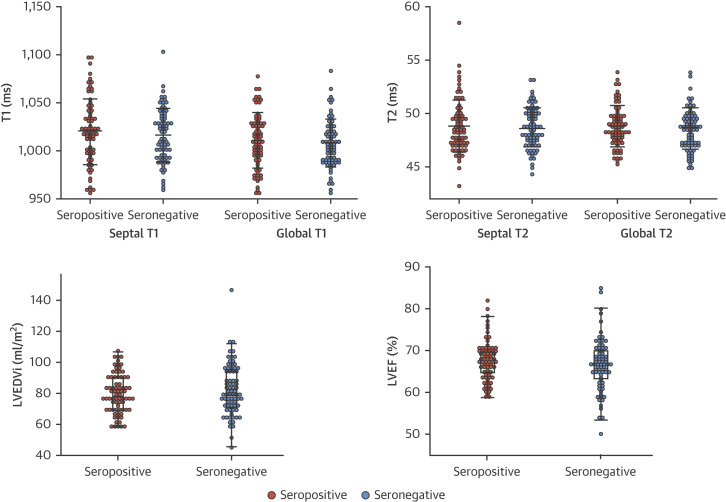
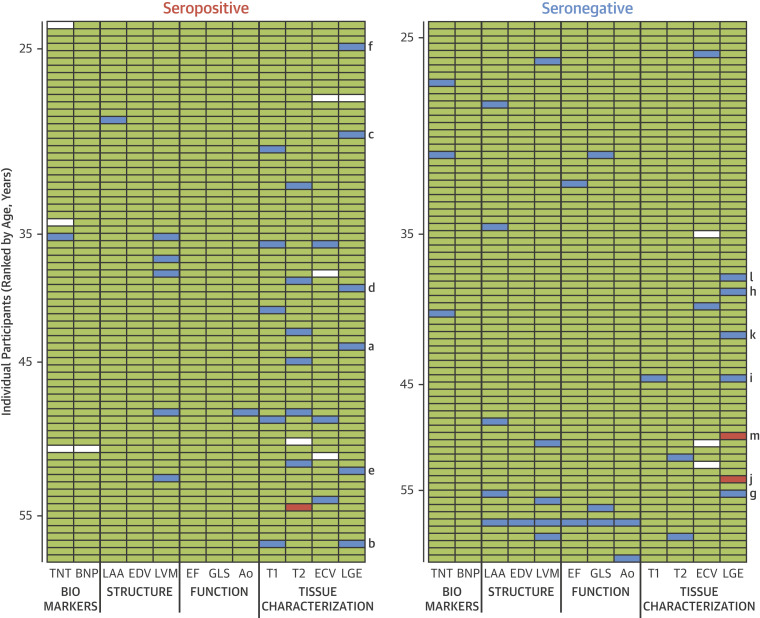
Results: A total of 149 subjects (mean age 37 years, range 18 to 63 years, 58% women) were recruited. Seropositive infections had been mild with case definition, noncase definition, and asymptomatic disease in 45 (61%), 18 (24%), and 11 (15%), respectively, with 1 person hospitalized (for 2 days). Between seropositive and seronegative groups, there were no differences in cardiac structure (left ventricular volumes, mass, atrial area), function (ejection fraction, global longitudinal shortening, aortic distensibility), tissue characterization (T1, T2, extracellular volume fraction mapping, late gadolinium enhancement) or biomarkers (troponin, N-terminal pro-B-type natriuretic peptide). With abnormal defined by the 75 seronegatives (2 SDs from mean, e.g., ejection fraction <54%, septal T1 >1,072 ms, septal T2 >52.4 ms), individuals had abnormalities including reduced ejection fraction (n = 2, minimum 50%), T1 elevation (n = 6), T2 elevation (n = 9), late gadolinium enhancement (n = 13, median 1%, max 5% of myocardium), biomarker elevation (borderline troponin elevation in 4; all N-terminal pro-B-type natriuretic peptide normal). These were distributed equally between seropositive and seronegative individuals.
Conclusions: Cardiovascular abnormalities are no more common in seropositive versus seronegative otherwise healthy, workforce representative individuals 6 months post-mild severe acute respiratory syndrome-coronavirus-2 infection.
Keywords: COVID-19; SARS-CoV-2; cardiovascular magnetic resonance; late gadolinium enhancement; myocardial edema; myocarditis; troponin.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures COVIDsortium funding was donated by individuals, charitable trusts, and corporations including Goldman Sachs, Citadel and Citadel Securities, The Guy Foundation, GW Pharmaceuticals, Kusuma Trust, and Jagclif Charitable Trust, and enabled by Barts Charity with support from UCLH Charity. Wider support is acknowledged on the COVIDsortium web site. Institutional support from Barts Health NHS Trust and Royal Free NHS Foundation Trust facilitated study processes, in partnership with University College London and Queen Mary University London. Serology tests (anti-S1 and anti-NP) were funded by Public Health England. This study forms part of the portfolio of COVID-Heart, a UKRI UKRI-DHSC funded study (ISRCTN58667920). The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report. Dr Seraphim is supported by a doctoral research fellowship from the British Heart Foundation (FS/18/83/34025). Dr Augusto is supported by an EACVI grant. Prof. McKnight is supported by Rosetrees trust, The John Black Charitable Foundation, and Medical College of St. Bartholomew’s Hospital Trust. Prof. Noursadeghi is supported by the Wellcome Trust (207511/Z/17/Z) and by NIHR Biomedical Research Funding to UCL and UCLH. Prof. Fontana is supported by a BHF Intermediate Research Fellowship (FS FS/18/21/33447). Dr Treibel is funded by a BHF Intermediate Research Fellowship (FS/19/35/34374). Drs Treibel and Manisty and Prof. Moon are directly and indirectly supported by the University College London Hospitals (UCLH) and Barts NIHR Biomedical Research Centres and through the British Heart Foundation (BHF) Accelerator Award (AA/18/6/34223). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Cardiovascular Complications Are Uncommon in Healthcare Workers With Mild or Asymptomatic COVID-19 Infection.JACC Cardiovasc Imaging. 2021 Nov;14(11):2167-2169. doi: 10.1016/j.jcmg.2021.04.022. Epub 2021 May 8. JACC Cardiovasc Imaging. 2021. PMID: 34119431 Free PMC article.
References
-
- Moore J.B., June C.H. Cytokine release syndrome in severe COVID-19. Science. 2020;368:473–474. - PubMed
-
- Liu P.P., Blet A., Smyth D., Li H. The science underlying COVID-19: implications for the cardiovascular system. Circulation. 2020;142:68–78. - PubMed
-
- Long B., Long D.A., Tannenbaum L., Koyfman A. An emergency medicine approach to troponin elevation due to causes other than occlusion myocardial infarction. Am J Emerg Med. 2020;38:998–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
