

Targeting Treg cells with GITR activation alleviates resistance to immunotherapy in murine glioblastomas
- PMID: 33976133
- PMCID: PMC8113440
- DOI: 10.1038/s41467-021-22885-8
Targeting Treg cells with GITR activation alleviates resistance to immunotherapy in murine glioblastomas
Abstract
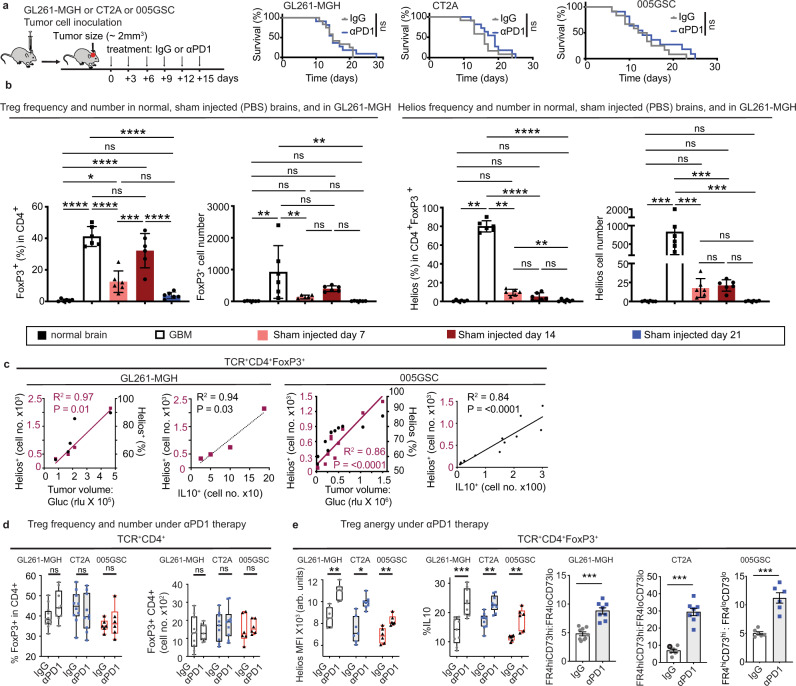
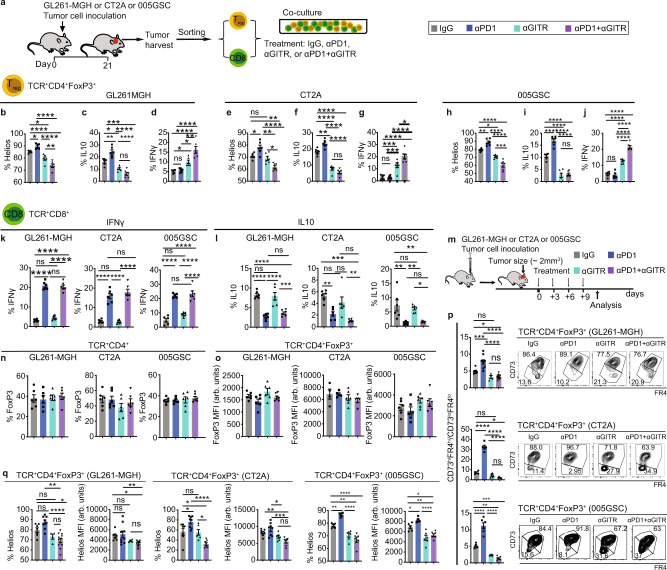
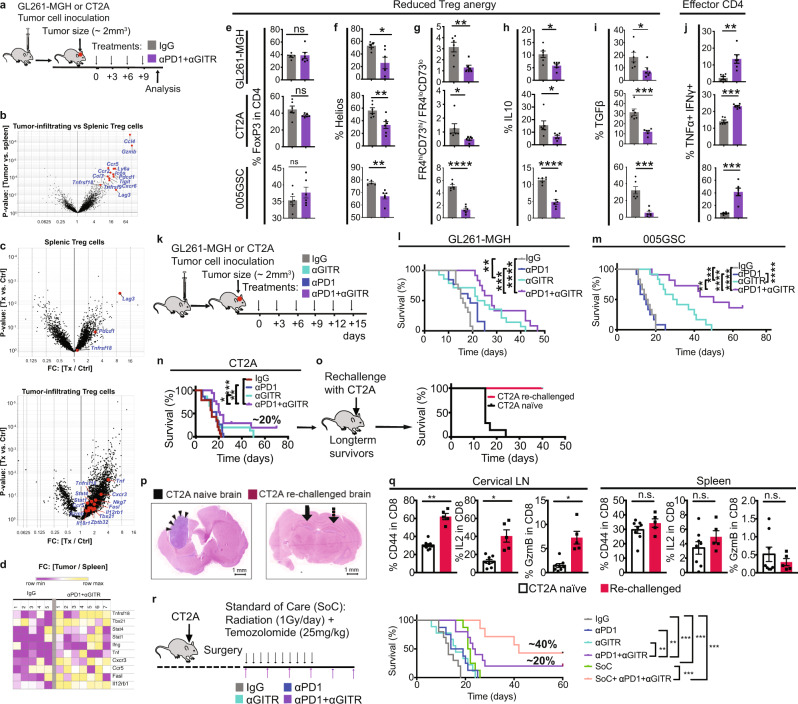
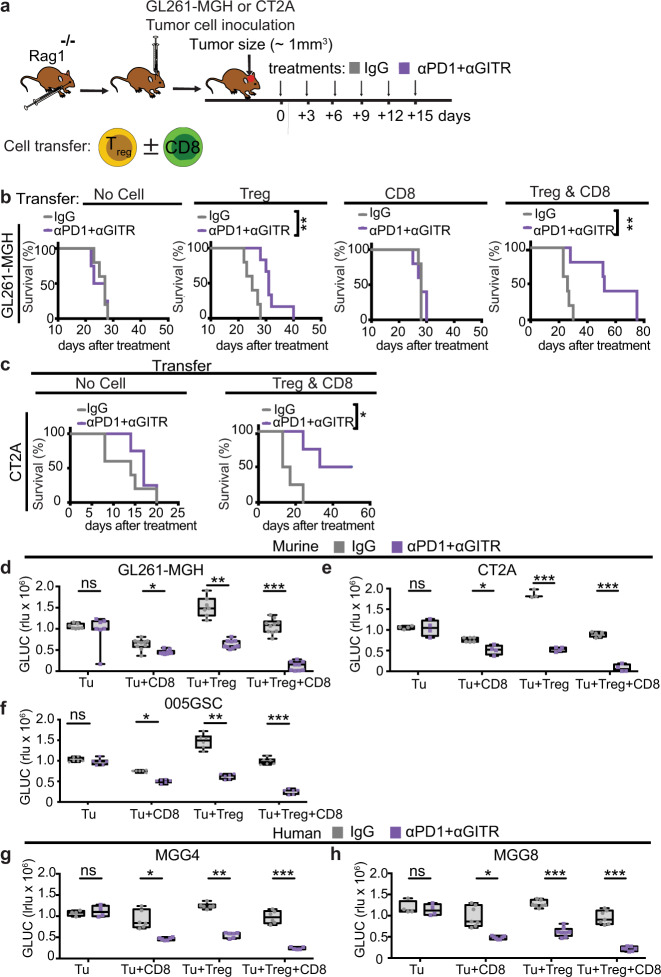
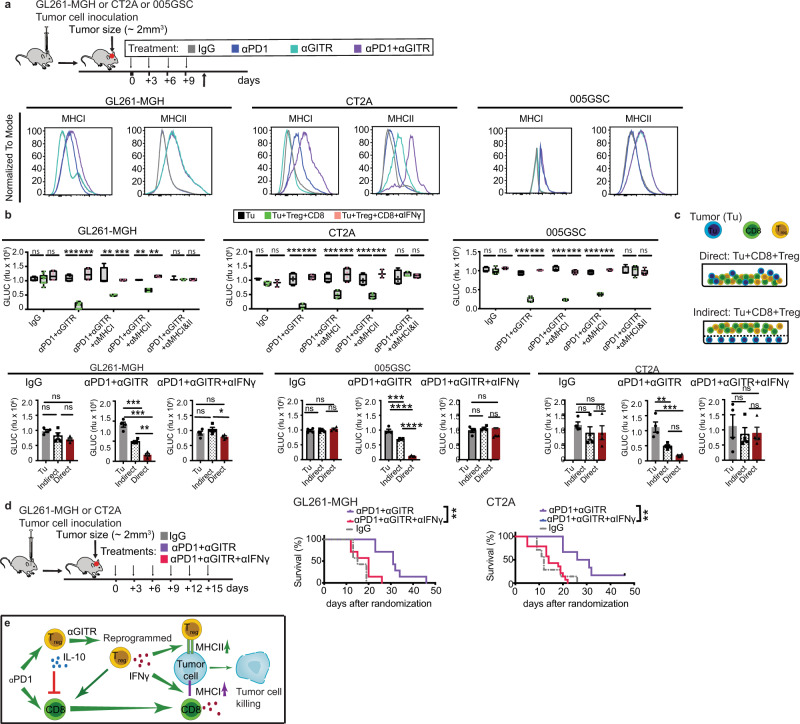
Immune checkpoint blockers (ICBs) have failed in all phase III glioblastoma (GBM) trials. Here, we show that regulatory T (Treg) cells play a key role in GBM resistance to ICBs in experimental gliomas. Targeting glucocorticoid-induced TNFR-related receptor (GITR) in Treg cells using an agonistic antibody (αGITR) promotes CD4 Treg cell differentiation into CD4 effector T cells, alleviates Treg cell-mediated suppression of anti-tumor immune response, and induces potent anti-tumor effector cells in GBM. The reprogrammed GBM-infiltrating Treg cells express genes associated with a Th1 response signature, produce IFNγ, and acquire cytotoxic activity against GBM tumor cells while losing their suppressive function. αGITR and αPD1 antibodies increase survival benefit in three experimental GBM models, with a fraction of cohorts exhibiting complete tumor eradication and immune memory upon tumor re-challenge. Moreover, αGITR and αPD1 synergize with the standard of care treatment for newly-diagnosed GBM, enhancing the cure rates in these GBM models.
Conflict of interest statement
R.K.J. received an honorarium from Amgen; consultant fees from Chugai, Merck, Ophthotech, Pfizer, SPARC, SynDevRx, XTuit; owns equity in Accurius, Elpis, Enlight, and SynDevRx; and serves on the Boards of Trustees of Tekla Healthcare Investors, Tekla Life Sciences Investors, Tekla Healthcare Opportunities Fund, Tekla World Healthcare Fund, and a grant from Boehringer Ingelheim. A.K.S. received compensation for consulting and/or SAB membership from Merck, Honeycomb Biotechnologies, Cellarity, Cogen Therapeutics and Dahlia Biosciences. No reagents or funding from these organizations was used in this study. The other authors have no competing interests to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 NS118929/NS/NINDS NIH HHS/United States
- U01 CA224348/CA/NCI NIH HHS/United States
- P01 CA080124/CA/NCI NIH HHS/United States
- R01 CA208205/CA/NCI NIH HHS/United States
- R01 CA082308/CA/NCI NIH HHS/United States
- P30 CA006516/CA/NCI NIH HHS/United States
- P01 CA119070/CA/NCI NIH HHS/United States
- P01 DE014388/DE/NIDCR NIH HHS/United States
- T32 HL007627/HL/NHLBI NIH HHS/United States
- P50 CA168504/CA/NCI NIH HHS/United States
- P01 CA092625/CA/NCI NIH HHS/United States
- T32 CA251062/CA/NCI NIH HHS/United States
- K12 CA090354/CA/NCI NIH HHS/United States
- R01 AI037562/AI/NIAID NIH HHS/United States
- R35 CA197743/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
