

A machine learning model for identifying patients at risk for wild-type transthyretin amyloid cardiomyopathy
- PMID: 33976166
- PMCID: PMC8113237
- DOI: 10.1038/s41467-021-22876-9
A machine learning model for identifying patients at risk for wild-type transthyretin amyloid cardiomyopathy
Abstract
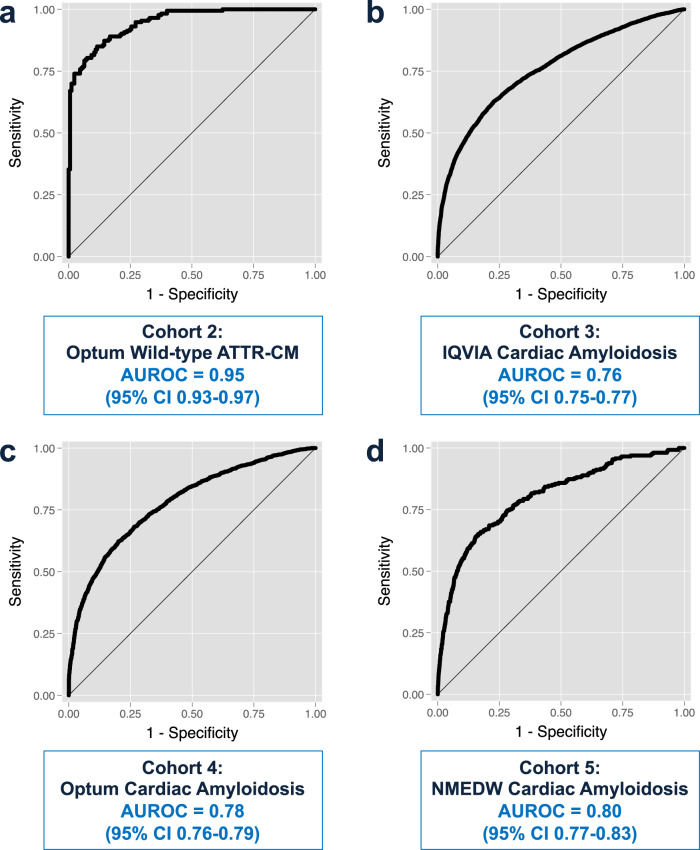
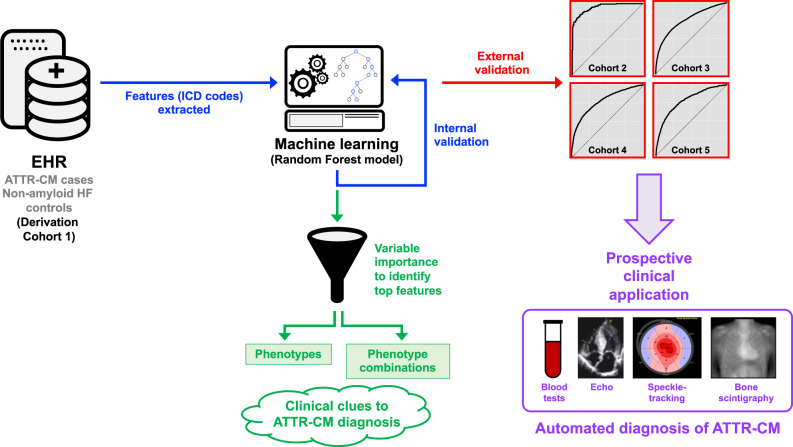
Transthyretin amyloid cardiomyopathy, an often unrecognized cause of heart failure, is now treatable with a transthyretin stabilizer. It is therefore important to identify at-risk patients who can undergo targeted testing for earlier diagnosis and treatment, prior to the development of irreversible heart failure. Here we show that a random forest machine learning model can identify potential wild-type transthyretin amyloid cardiomyopathy using medical claims data. We derive a machine learning model in 1071 cases and 1071 non-amyloid heart failure controls and validate the model in three nationally representative cohorts (9412 cases, 9412 matched controls), and a large, single-center electronic health record-based cohort (261 cases, 39393 controls). We show that the machine learning model performs well in identifying patients with cardiac amyloidosis in the derivation cohort and all four validation cohorts, thereby providing a systematic framework to increase the suspicion of transthyretin cardiac amyloidosis in patients with heart failure.
Conflict of interest statement
S.J.S. has received grants from Actelion, AstraZeneca, Corvia, Novartis, and Pfizer; and has received consulting fees from Actelion, Amgen, AstraZeneca, Bayer, Boehringer-Ingelheim, Cardiora, Eisai, Ionis, Ironwood, Merck, Novartis, Pfizer, Sanofi, and United Therapeutics. R.C.D. has received a grant from GE Healthcare and has received consulting fees from Novartis and Pfizer. A.C., M.B., A.H., A.N., M.S., and J.S. are full-time employees of Pfizer. All other authors report no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
