

Multimodal integrated approaches in low grade glioma surgery
- PMID: 33976246
- PMCID: PMC8113473
- DOI: 10.1038/s41598-021-87924-2
Multimodal integrated approaches in low grade glioma surgery
Abstract
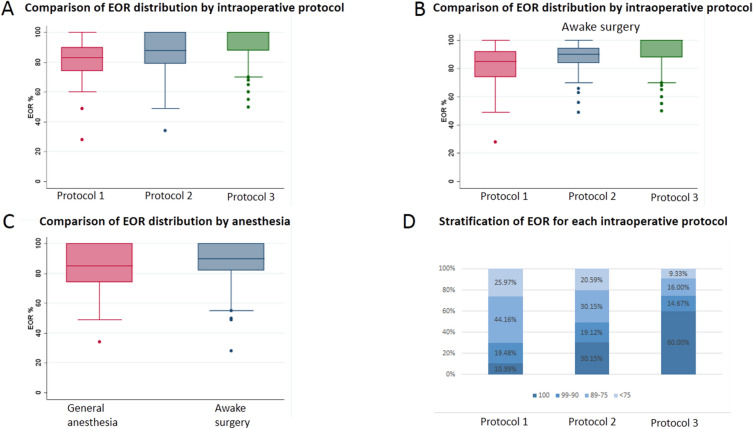
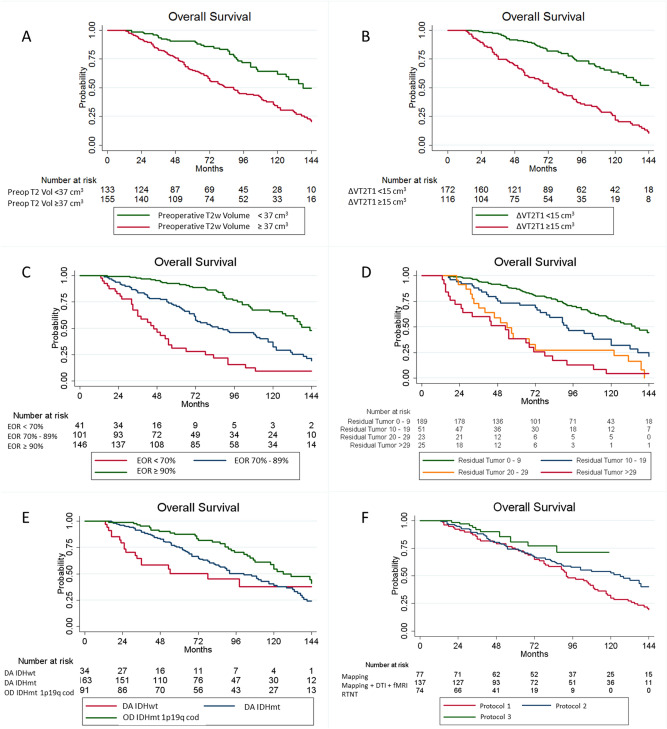
Surgical management of Diffuse Low-Grade Gliomas (DLGGs) has radically changed in the last 20 years. Awake surgery (AS) in combination with Direct Electrical Stimulation (DES) and real-time neuropsychological testing (RTNT) permits continuous intraoperative feedback, thus allowing to increase the extent of resection (EOR). The aim of this study was to evaluate the impact of the technological advancements and integration of multidisciplinary techniques on EOR. Two hundred and eighty-eight patients affected by DLGG were enrolled. Cases were stratified according to the surgical protocol that changed over time: 1. DES; 2. DES plus functional MRI/DTI images fused on a NeuroNavigation system; 3. Protocol 2 plus RTNT. Patients belonging to Protocol 1 had a median EOR of 83% (28-100), while those belonging to Protocol 2 and 3 had a median EOR of 88% (34-100) and 98% (50-100) respectively (p = 0.0001). New transient deficits with Protocol 1, 2 and 3 were noted in 38.96%, 34.31% and 31,08% of cases, and permanent deficits in 6.49%, 3.65% and 2.7% respectively. The average follow-up period was 6.8 years. OS was influenced by molecular class (p = 0.028), EOR (p = 0.018) and preoperative tumor growing pattern (p = 0.004). Multimodal surgical approach can provide a safer and wider removal of DLGG with potential subsequent benefits on OS. Further studies are necessary to corroborate our findings.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
