

Multi-step screening of neoantigens' HLA- and TCR-interfaces improves prediction of survival
- PMID: 33976291
- PMCID: PMC8113358
- DOI: 10.1038/s41598-021-89016-7
Multi-step screening of neoantigens' HLA- and TCR-interfaces improves prediction of survival
Abstract
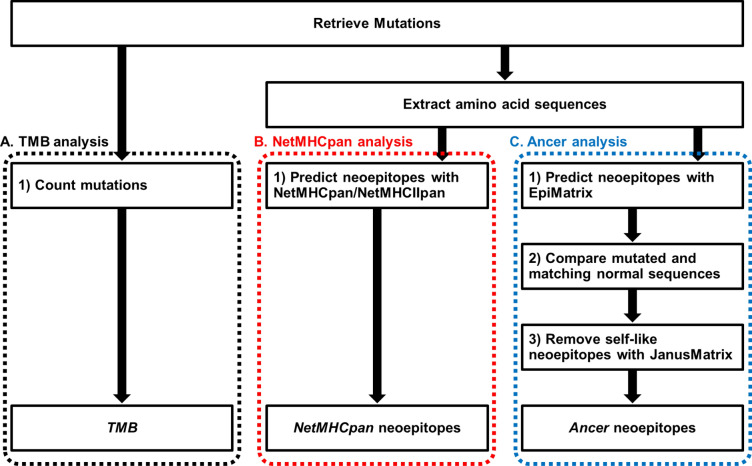
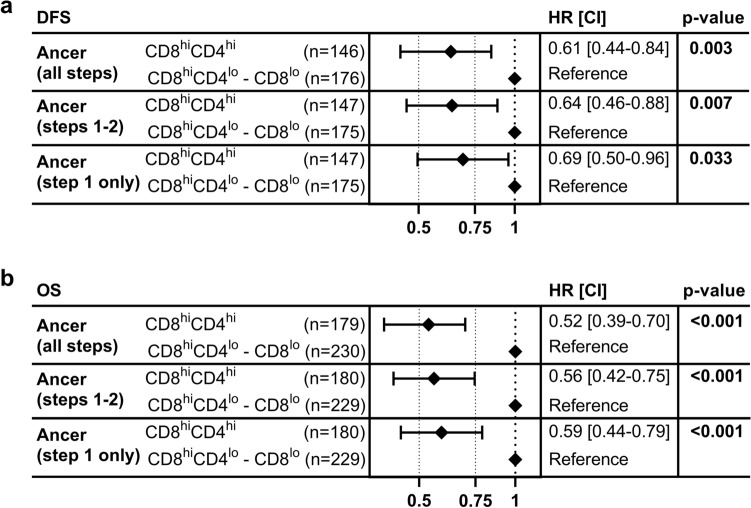
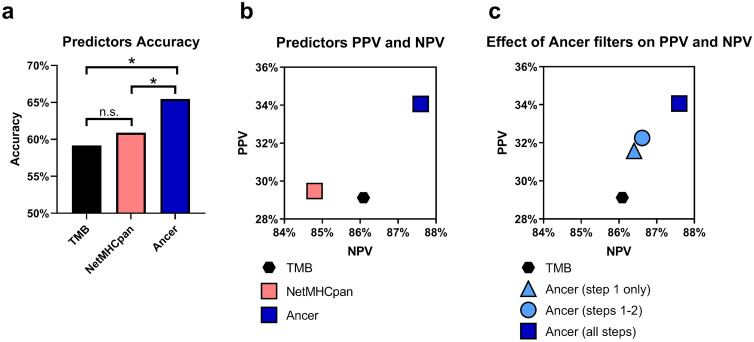
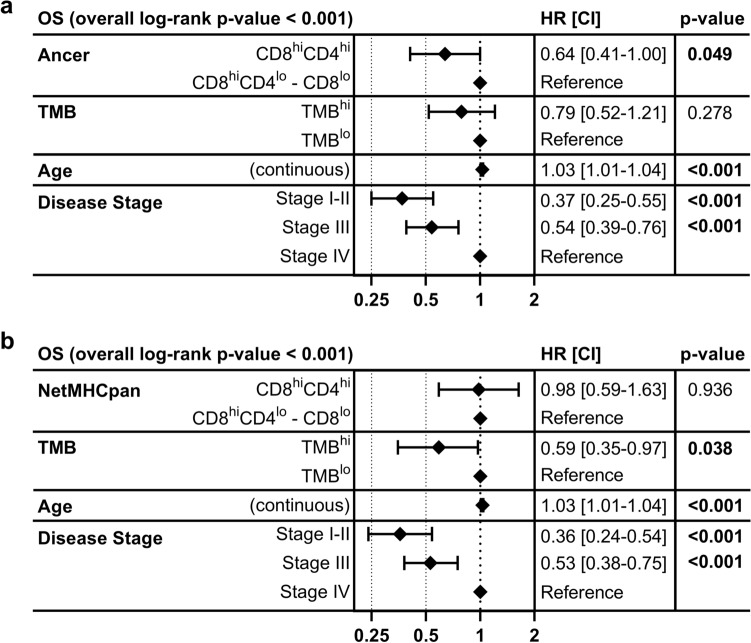
Improvement of risk stratification through prognostic biomarkers may enhance the personalization of cancer patient monitoring and treatment. We used Ancer, an immunoinformatic CD8, CD4, and regulatory T cell neoepitope screening system, to perform an advanced neoantigen analysis of genomic data derived from the urothelial cancer cohort of The Cancer Genome Atlas. Ancer demonstrated improved prognostic stratification and five-year survival prediction compared to standard analyses using tumor mutational burden or neoepitope identification using NetMHCpan and NetMHCIIpan. The superiority of Ancer, shown in both univariate and multivariate survival analyses, is attributed to the removal of neoepitopes that do not contribute to tumor immunogenicity based on their homology with self-epitopes. This analysis suggests that the presence of a higher number of unique, non-self CD8- and CD4-neoepitopes contributes to cancer survival, and that prospectively defining these neoepitopes using Ancer is a novel prognostic or predictive biomarker.
Conflict of interest statement
ADG and WDM are senior officers and majority shareholders, and MA is an employee of EpiVax, Inc, a privately owned immunoinformatics and vaccine design company. All three of these authors are also involved in developing the Ancer pipeline. These authors acknowledge that there is a potential conflict of interest related to their relationship with EpiVax and attest that the work contained in this research report is free of any bias that might be associated with the commercial goals of the company. GB was previously a senior officer of EpiVax Therapeutics, Inc., MFP is a senior officer and GR is currently an employee of EpiVax Therapeutics, Inc., a precision immunotherapy company and subsidiary of EpiVax, Inc. MFP and GR have equity in EpiVax Therapeutics. These authors acknowledge that there is a potential conflict of interest related to their relationship with EpiVax Therapeutics and attest that the work contained in this research report is free of any bias that might be associated with the commercial goals of the company. EpiVax, Inc. and EpiVax Therapeutics, Inc. own patents to technologies utilized by associated authors in the research reported here. RFS reports honoraria from Aduro, AstraZeneca, BMS, Exelixis, Eisai, Janssen, Mirati, Pfizer, and Puma. GDS is a member of Clinical Trial Protocol Committees for the following companies: Merck, BMS, Janssen, Cold Genesys, Pfizer, PhotoCure, Fidia, is or has been a scientific advisor/consultant within the past 5 years for the following companies: Heat Biologics, Cold Genesys, PhotoCure, Merck, Roche/Genentech, Ciclomed, Taris Biomedical, MDxHealth, Fidia Farmaceuticals, Urogen, Ferring, Aduro, Boston Scientific, Bristol Myers Squibb, Astra Zeneca, Pfizer, Janssen, EpiVax Therapeutics, Natera, FKD, Ferring, EnGene Bio, SesenBio, BioCanCell, Nucleix, Ipsen, Combat Medical, Astellas, Fergene, Dendreon, Abbvie, Seattle Genetics, and has equity stock/options in EpiVax Therapeutics and Urogen. AVB reports equity stock/options in EpiVax Therapeutics. TIG and AK declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
