

Second allogeneic transplants for multiple myeloma: a report from the EBMT Chronic Malignancies Working Party
- PMID: 33976382
- PMCID: PMC8486670
- DOI: 10.1038/s41409-021-01286-x
Second allogeneic transplants for multiple myeloma: a report from the EBMT Chronic Malignancies Working Party
Abstract
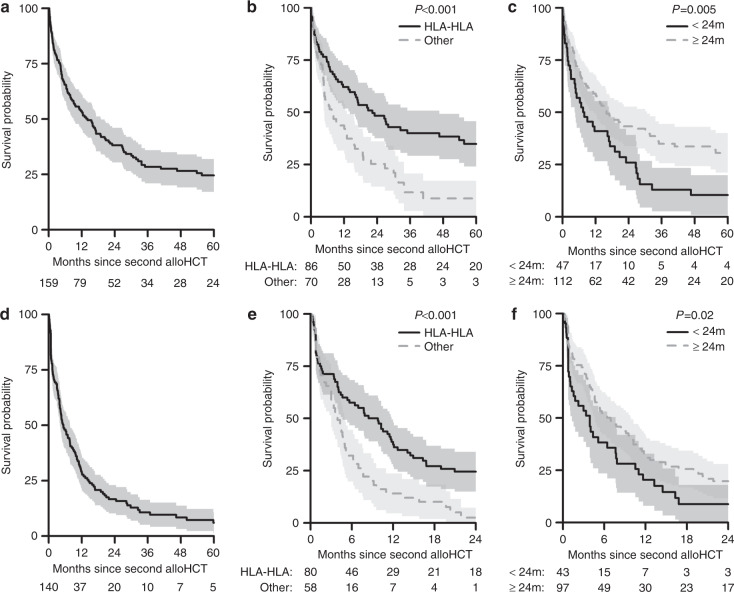
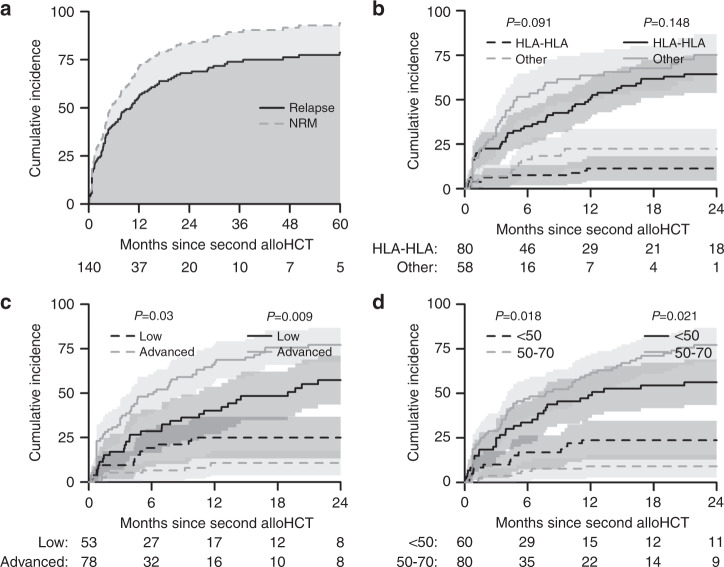
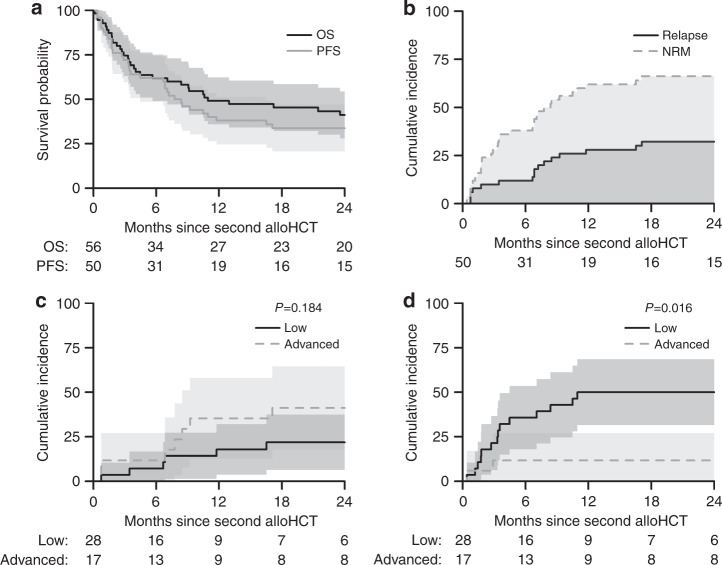
The EBMT Chronic Malignancies Working Party performed a retrospective analysis of 215 patients who underwent a second allo-HCT for myeloma between 1994 and 2017, 159 for relapse and 56 for graft failure. In the relapse group, overall survival (OS) was 38% (30-46%) at 2 years and 25% (17-32%) at 5 years. Patients who had a HLA-identical sibling (HLAid-Sib) donor for their first and second transplants had superior OS (5 year OS: HLAid-Sib/HLAid-Sib: 35% (24-46%); Others 9% (0-17%), p < 0.001). There was a significantly higher incidence of acute grade II-IV GvHD in those patients who had also developed GvHD following their initial HLA-identical sibling allo-HCT (HLAid-Sib/HLAid-Sib: 50% (33-67%); Other 22% (8-36%), p = 0.03). More as opposed to fewer than 2 years between transplants was associated with superior 5-yr OS (31% (21-40%) vs. 10% (1-20%), P = 0.005). On multivariate analysis, consecutive HLA-identical sibling donor transplants conferred a significant OS advantage (0.4 (0.24-0.67), p < 0.001). In the graft failure group, OS was 41% at 2 years. In summary, a second allo-HCT using a HLA-identical sibling donor, if available, provides the best transplant outcomes for relapsed myeloma in this setting.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Chen YB, McCarthy PL, Hahn T, Holstein SA, Ueda M, Kroger N, et al. Methods to prevent and treat relapse after hematopoietic stem cell transplantation with tyrosine kinase inhibitors, immunomodulating drugs, deacetylase inhibitors, and hypomethylating agents. Bone Marrow Transpl. 2019;54:497–507. doi: 10.1038/s41409-018-0269-3. - DOI - PubMed
-
- Shaw BE, Mufti GJ, Mackinnon S, Cavenagh JD, Pearce RM, Towlson KE, et al. Outcome of second allogeneic transplants using reduced-intensity conditioning following relapse of haematological malignancy after an initial allogeneic transplant. Bone Marrow Transpl. 2008;42:783–9. doi: 10.1038/bmt.2008.255. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
