

Intra-Coronary Administration of Tacrolimus Improves Myocardial Perfusion and Left Ventricular Function in Patients with ST-Segment Elevation Myocardial Infarction (COAT-STEMI) Undergoing Primary Percutaneous Coronary Intervention
- PMID: 33976507
- PMCID: PMC8107710
- DOI: 10.6515/ACS.202105_37(3).20201025C
Intra-Coronary Administration of Tacrolimus Improves Myocardial Perfusion and Left Ventricular Function in Patients with ST-Segment Elevation Myocardial Infarction (COAT-STEMI) Undergoing Primary Percutaneous Coronary Intervention
Abstract
Background: Ischemia-reperfusion injury following acute ST-segment elevation myocardial infarction (STEMI) is strongly related to inflammation. However, whether intracoronary (IC) tacrolimus, an immunosuppressant, can improve myocardial perfusion is uncertain.
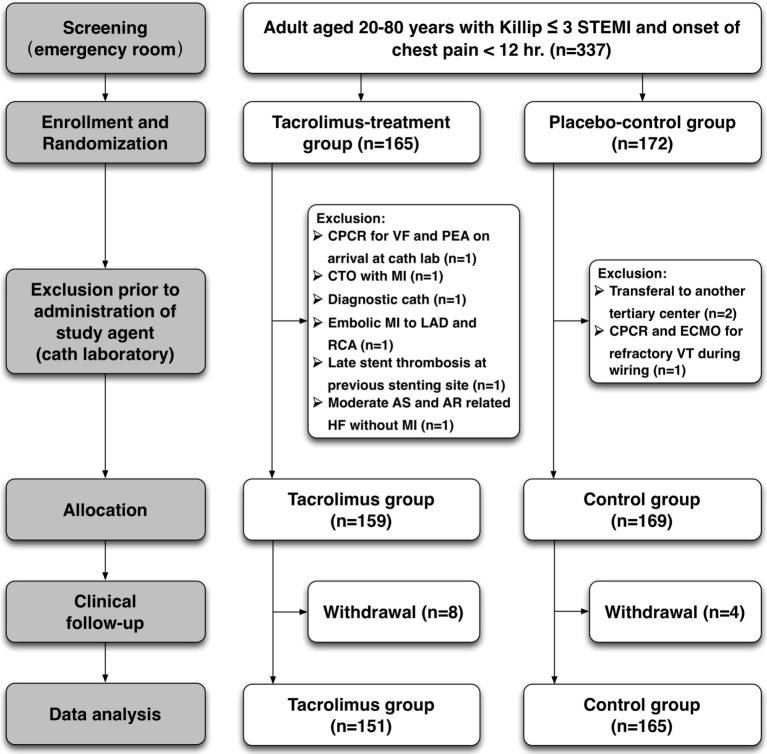
Methods: A multicenter double-blind randomized controlled trial was conducted in Taiwan from 2014 to 2017. Among 316 STEMI patients with Killip class ≤ 3 undergoing primary percutaneous coronary intervention (PCI), 151 were assigned to the study group treated with IC tacrolimus 2.5 mg to the culprit vessel before first balloon inflation, and the remaining 165 were assigned to the placebo group receiving IC saline only. The primary endpoint was percentage of post-PCI TIMI-3 flow. The primary composite endpoints included achievement of TIMI-3 flow, TIMI- myocardial perfusion (TMP) grade, or 90-min ST-segment resolution (STR). The secondary endpoints were left ventricular ejection fraction (LVEF) and 1-month/1-year major adverse cardio-cerebral vascular events (MACCEs) (defined as death, myocardial infarction, stroke, target-vessel revascularization or re-hospitalization for heart failure).
Results: Although post-PCI TIMI-3 epicardial flow and MACCE rate at 1 month and 1 year did not differ between the two groups, TMP grade (2.54 vs. 2.23, p < 0.001) and 90-min STR (67% vs. 61%, p < 0.001) were significantly higher in the tacrolimus-treated group than in the placebo group. The STEMI patients treated with tacrolimus also had significantly higher 3D LVEF and less grade 2 or 3 LV diastolic dysfunction at 9 months compared to those without.
Conclusions: IC tacrolimus for STEMI improved coronary microcirculation and 9-month LV systolic and diastolic functions. However, the benefit of tacrolimus on clinical outcomes remains inconclusive due to insufficient patient enrollment.
Keywords: Left ventricular systolic and diastolic function; Microcirculation; Myocardial perfusion; ST-segment elevation myocardial infarction; Tacrolimus.
Figures



Similar articles
-
[Effects of pretreatment with recombinant human B-type natriuretic peptide on infarct size in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention].Zhonghua Xin Xue Guan Bing Za Zhi. 2015 Nov;43(11):954-9. Zhonghua Xin Xue Guan Bing Za Zhi. 2015. PMID: 26888806 Clinical Trial. Chinese.
-
Clinical benefits of adjunctive tirofiban therapy in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention.Coron Artery Dis. 2008 Jun;19(4):271-7. doi: 10.1097/MCA.0b013e3282f487e0. Coron Artery Dis. 2008. PMID: 18480672 Clinical Trial.
-
Comparison between the Outcomes of Intracoronary and Intravenous Administration of Eptifibatide during Primary Percutaneous Coronary Intervention in Patients with Acute ST-Elevation Myocardial Infarction.J Atheroscler Thromb. 2016;23(4):465-76. doi: 10.5551/jat.30965. Epub 2015 Dec 2. J Atheroscler Thromb. 2016. PMID: 26632161 Clinical Trial.
-
Remote ischemic conditioning during primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction: a systematic review and meta-analysis.J Cardiothorac Surg. 2019 Jan 21;14(1):14. doi: 10.1186/s13019-019-0834-x. J Cardiothorac Surg. 2019. PMID: 30696461 Free PMC article.
-
Safety and efficacy of intracoronary adenosine administration in patients with acute myocardial infarction undergoing primary percutaneous coronary intervention: a meta-analysis of randomized controlled trials.Ther Adv Cardiovasc Dis. 2012 Jun;6(3):101-14. doi: 10.1177/1753944712446670. Epub 2012 May 4. Ther Adv Cardiovasc Dis. 2012. PMID: 22562999 Review.
Cited by
-
Trends, Clinical Characteristics, and Outcomes of Percutaneous Coronary Intervention in Liver Transplant Recipients.Clin Transplant. 2025 May;39(5):e70181. doi: 10.1111/ctr.70181. Clin Transplant. 2025. PMID: 40373057 Free PMC article.
-
Combined tacrolimus and melatonin effectively protected kidney against acute ischemia-reperfusion injury.FASEB J. 2021 Jun;35(6):e21661. doi: 10.1096/fj.202100174R. FASEB J. 2021. PMID: 34029398 Free PMC article.
-
Safety and efficacy of intracoronary artery administration of human bone marrow-derived mesenchymal stem cells in STEMI of Lee-Sung pigs-A preclinical study for supporting the feasibility of the OmniMSC-AMI phase I clinical trial.Front Cardiovasc Med. 2023 Mar 29;10:1153428. doi: 10.3389/fcvm.2023.1153428. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37063964 Free PMC article.
References
-
- Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327:669–677. - PubMed
-
- Yip HK, Wu CJ, Chang HW, et al. Comparison of impact of primary percutaneous transluminal coronary angioplasty and primary stenting on short-term mortality in patients with cardiogenic shock and evaluation of prognostic determinants. Am J Cardiol. 2001;87:1184–1188; a1184. - PubMed
-
- Michaels AD, Gibson CM, Barron HV. Microvascular dysfunction in acute myocardial infarction: focus on the roles of platelet and inflammatory mediators in the no-reflow phenomenon. Am J Cardiol. 2000;85:50b–60b. - PubMed
-
- Yip HK, Wu CJ, Chang HW, et al. Effect of the PercuSurge GuardWire device on the integrity of microvasculature and clinical outcomes during primary transradial coronary intervention in acute myocardial infarction. Am J Cardiol. 2003;92:1331–1335. - PubMed
-
- Yip HK, Chen MC, Chang HW, et al. Angiographic morphologic features of infarct-related arteries and timely reperfusion in acute myocardial infarction: predictors of slow-flow and no-reflow phenomenon. Chest. 2002;122:1322–1332. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous