

Functional Testing for Tranexamic Acid Duration of Action Using Modified Viscoelastometry
- PMID: 33976611
- PMCID: PMC8077595
- DOI: 10.1159/000511230
Functional Testing for Tranexamic Acid Duration of Action Using Modified Viscoelastometry
Abstract
Introduction: Tranexamic acid (TXA) is the standard medication to prevent or treat hyperfibrinolysis. However, prolonged inhibition of lysis (so-called "fibrinolytic shutdown") correlates with increased mortality. A new viscoelastometric test enables bedside quantification of the antifibrinolytic activity of TXA using tissue plasminogen activator (TPA).
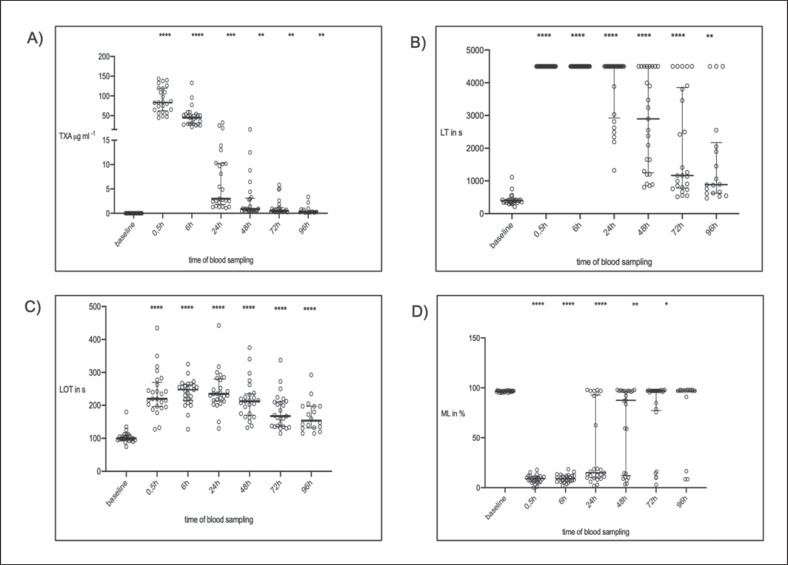
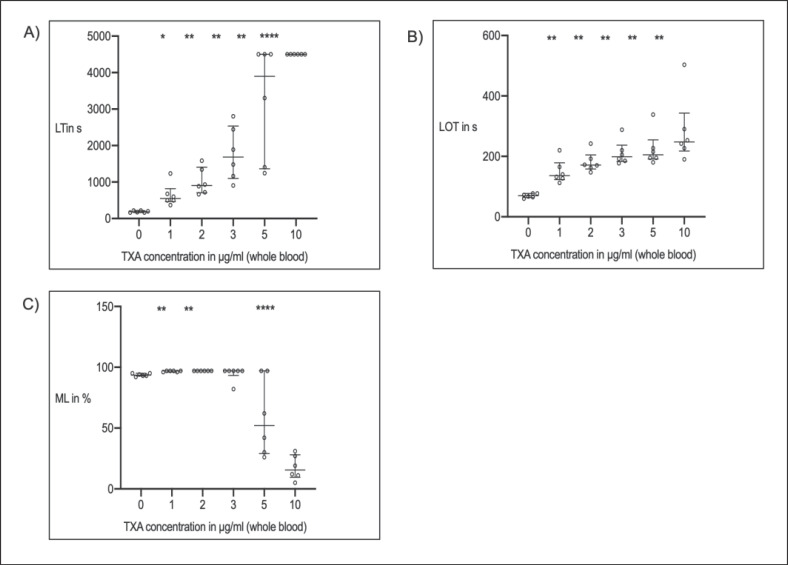
Materials and methods: Twenty-five cardiac surgery patients were included in this prospective observational study. In vivo, the viscoelastometric TPA test was used to determine lysis time (LT) and maximum lysis (ML) over 96 h after TXA bolus. Additionally, plasma concentrations of TXA and plasminogen activator inhibitor 1 (PAI-1) were measured. Moreover, dose effect curves from the blood of healthy volunteers were performed in vitro. Data are presented as median (25-75th percentile).
Results: In vivo TXA plasma concentration correlated with LT (r = 0.55; p < 0.0001) and ML (r = 0.62; p < 0.0001) at all time points. Lysis was inhibited up to 96 h (LTTPA-test: baseline: 398 s [229-421 s] vs. at 96 h: 886 s [626-2,175 s]; p = 0.0013). After 24 h, some patients (n = 8) had normalized lysis, but others (n = 17) had strong lysis inhibition (ML <30%; p < 0.001). The high- and low-lysis groups differed regarding kidney function (cystatin C: 1.64 [1.42-2.02] vs. 1.28 [1.01-1.52] mg/L; p = 0.002) in a post hoc analysis. Of note, TXA plasma concentration after 24 h was significantly higher in patients with impaired renal function (9.70 [2.89-13.45] vs.1.41 [1.30-2.34] µg/mL; p < 0.0001). In vitro, TXA concentrations of 10 µg/mL effectively inhibited fibrinolysis in all blood samples.
Conclusions: Determination of antifibrinolytic activity using the TPA test is feasible, and individual fibrinolytic capacity, e.g., in critically ill patients, can potentially be measured. This is of interest since TXA-induced lysis inhibition varies depending on kidney function.
Keywords: Cardiac surgery; Fibrinolysis shutdown; Hyperfibrinolysis; Thromboelastometry; Tranexamic acid; Viscoelastometry.
Copyright © 2020 by S. Karger AG, Basel.
Conflict of interest statement
The authors declare there are no competing interests.
Figures
Similar articles
-
Functional testing of tranexamic acid effects in patients undergoing elective orthopaedic surgery.J Thromb Thrombolysis. 2021 May;51(4):989-996. doi: 10.1007/s11239-020-02272-8. Epub 2020 Sep 12. J Thromb Thrombolysis. 2021. PMID: 32918670
-
Point-of-care testing for tranexamic acid efficacy: a proof-of-concept study in cardiac surgical patients.Br J Anaesth. 2024 Jun;132(6):1211-1218. doi: 10.1016/j.bja.2024.03.023. Epub 2024 Apr 26. Br J Anaesth. 2024. PMID: 38677950
-
Effective tranexamic acid concentration for 95% inhibition of tissue-type plasminogen activator induced hyperfibrinolysis in children with congenital heart disease: A prospective, controlled, in-vitro study.Eur J Anaesthesiol. 2015 Dec;32(12):844-50. doi: 10.1097/EJA.0000000000000316. Eur J Anaesthesiol. 2015. PMID: 26258658
-
Application of a plasmin generation assay to define pharmacodynamic effects of tranexamic acid in women undergoing cesarean delivery.J Thromb Haemost. 2021 Jan;19(1):221-232. doi: 10.1111/jth.15114. Epub 2020 Dec 26. J Thromb Haemost. 2021. PMID: 33001565 Free PMC article.
-
The emerging role of tranexamic acid and its principal target, plasminogen, in skeletal health.Acta Pharm Sin B. 2024 Jul;14(7):2869-2884. doi: 10.1016/j.apsb.2024.03.033. Epub 2024 Mar 30. Acta Pharm Sin B. 2024. PMID: 39027253 Free PMC article. Review.
Cited by
-
Predictive ability of viscoelastic testing using ClotPro® for short-term outcome in patients with severe Covid-19 ARDS with or without ECMO therapy: a retrospective study.Thromb J. 2022 Aug 29;20(1):48. doi: 10.1186/s12959-022-00403-0. Thromb J. 2022. PMID: 36038895 Free PMC article.
-
[Tranexamic acid and arthroplasty: between off-label use and evidence-based medicine].Anaesthesist. 2021 Jul;70(7):614-615. doi: 10.1007/s00101-021-00989-6. Epub 2021 Jun 11. Anaesthesist. 2021. PMID: 34115141 Free PMC article. German. No abstract available.
-
[Standard administration of tranexamic acid for prophylaxis in endoprosthetics: a good idea?].Orthopade. 2022 Apr;51(4):337-338. doi: 10.1007/s00132-022-04236-7. Epub 2022 Mar 8. Orthopade. 2022. PMID: 35258633 German. No abstract available.
-
Are Viscoelastometric Assays of Old Generation Ready for Disposal? Comment on Volod et al. Viscoelastic Hemostatic Assays: A Primer on Legacy and New Generation Devices. J. Clin. Med. 2022, 11, 860.J Clin Med. 2023 Jan 6;12(2):477. doi: 10.3390/jcm12020477. J Clin Med. 2023. PMID: 36675406 Free PMC article.
-
Concentration-effect relationship for tranexamic acid inhibition of tissue plasminogen activator-induced fibrinolysis in vitro using the viscoelastic ClotPro® TPA-test.Br J Anaesth. 2024 Feb;132(2):343-351. doi: 10.1016/j.bja.2023.09.027. Epub 2023 Nov 3. Br J Anaesth. 2024. PMID: 37925268 Free PMC article.
References
-
- Kozek-Langenecker SA, Ahmed AB, Afshari A, Albaladejo P, Aldecoa C, Barauskas G, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology: First update 2016. Eur J Anaesthesiol. 2017 Jun;34((6)):332–95. - PubMed
-
- European Society of Anaesthesiology task force reports on place of aprotinin in clinical anaesthesia. Aprotinin: is it time to reconsider? Eur J Anaesthesiol. 2015 Sep;32((9)):591–5. - PubMed
-
- Nishijima DK, Kuppermann N, Roberts I, VanBuren JM, Tancredi DJ. The Effect of Tranexamic Acid on Functional Outcomes: An Exploratory Analysis of the CRASH-2 Randomized Controlled Trial. Ann Emerg Med. 2019 Jan;74((1)):79–87. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
