

Granulomatosis with Polyangiitis with Ocular Manifestations
- PMID: 33976664
- PMCID: PMC8077634
- DOI: 10.1159/000510959
Granulomatosis with Polyangiitis with Ocular Manifestations
Abstract
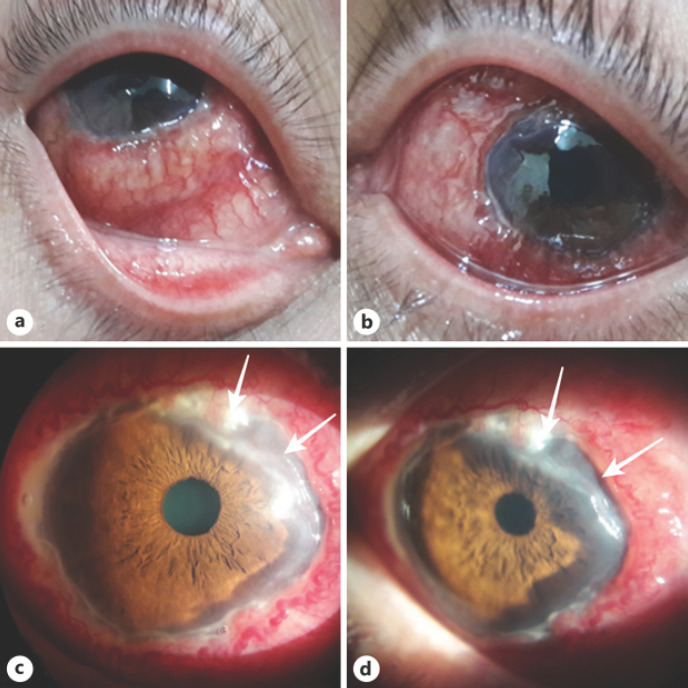
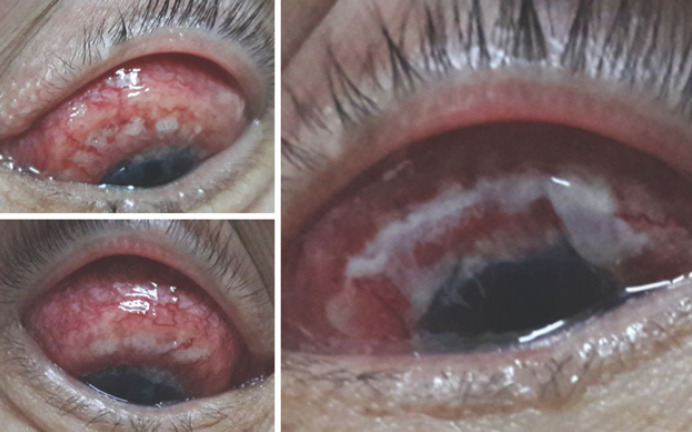
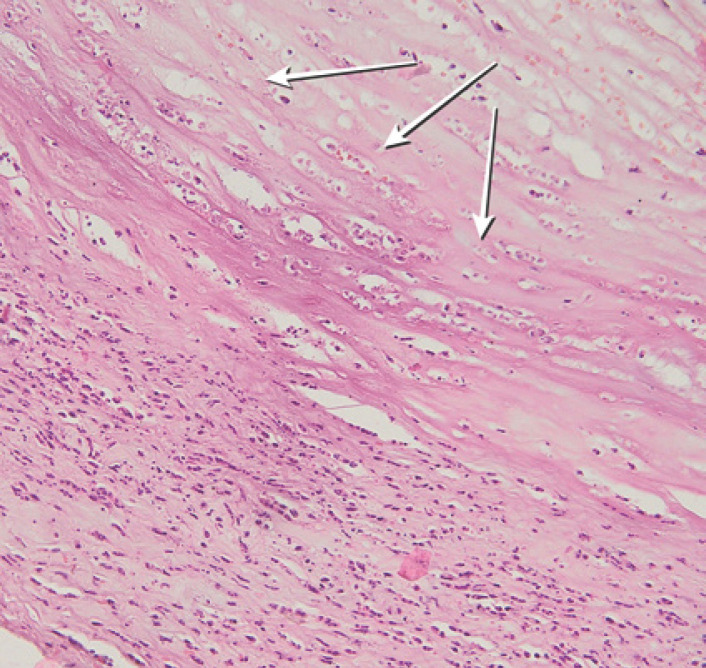
Granulomatosis with polyangiitis (GPA) is a granulomatous-necrotic systemic vasculitis with a lesion of predominantly the upper and lower respiratory tracts at the onset of the disease (vasculitis, accompanied by granulomatous inflammation), and subsequently renal (glomerulonephritis). In addition, GPA may manifest as inflammation of small arteries and veins. Despite many years of study of this disease, the etiology of GPA remains unknown. The present case is about a 47-year-old female, who had been suffering from necrotizing scleritis, corneal ulcer, and secondary glaucoma in both eyes for 3 months, and she was treated with anti-inflammatory and antimicrobial therapy that showed no effect; the patient's general condition became worse. In the second week of treatment, multiple abscess ruptures exposed the sclera. Sampling of the affected conjunctival tissue and positive HLA B8 haplotype and ANCA (PR3-ANCA) testings make it clear that GPA was the main reason of necrotizing scleritis with inflammation. The targeted treatment of the underlying disease allows to stabilize an inflammation of corneal and scleral lesions.
Keywords: Corneal ulcer; Granulomatosis with polyangiitis; Necrotizing scleritis; Wegener's granulomatosis.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


References
-
- Tarabishy AB, Schulte M, Papaliodis GN, Hoffman GS. Wegener's granulomatosis: clinical manifestations, differential diagnosis, and management of ocular and systemic disease. Surv Ophthalmol. 2010 Sep-Oct;55((5)):429–44. - PubMed
-
- Allen SD, Harvey CJ. Imaging of Wegener's granulomatosis. Br J Radiol. 2007 Sep;80((957)):757–65. - PubMed
-
- Kubal AA, Perez VL. Ocular manifestations of ANCA-associated vasculitis. Rheum Dis Clin North Am. 2010 Aug;36((3)):573–86. - PubMed
-
- Khan AR, Chapman PT, Stamp LK, Wells JE, O'Donnell JL. Wegener's granulomatosis: treatment and survival characteristics in a high-prevalence southern hemisphere region. Intern Med J. 2012 Apr;42((4)):e23–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
