

Time-Varying mHAP-III Is the Most Accurate Predictor of Survival in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization
- PMID: 33977089
- PMCID: PMC8077424
- DOI: 10.1159/000513404
Time-Varying mHAP-III Is the Most Accurate Predictor of Survival in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization
Abstract
Introduction: The prognosis of patients undergoing transarterial chemoembolization (TACE) is extremely variable, and a confounding factor is that TACE is often repeated several times. We retrospectively evaluated the accuracy of different prognostic scores and staging systems in estimating overall survival (OS) in patients with hepatocellular carcinoma (HCC).
Methods: An analysis considering prognostic models as time-varying variables was performed, calculating OS from the time of TACE to the time of the subsequent treatment. Total follow-up time for each patient was therefore split into several observation times accounting for each TACE procedure. Values of the likelihood ratio test (LRT) and Akaike information criterion (AIC) were used to compare different systems. Univariable and multivariable analyses were conducted to identify additional factors predictive of OS. We analyzed 1,610 TACE performed in 1,058 patients recorded in the Italian Liver Cancer database from 2008 through 2016.
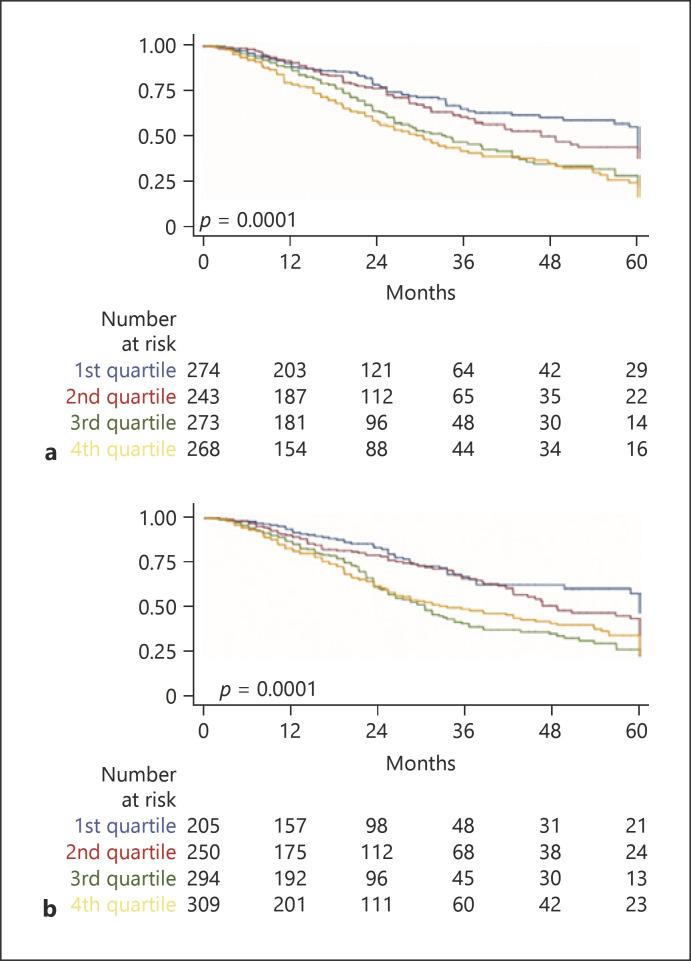
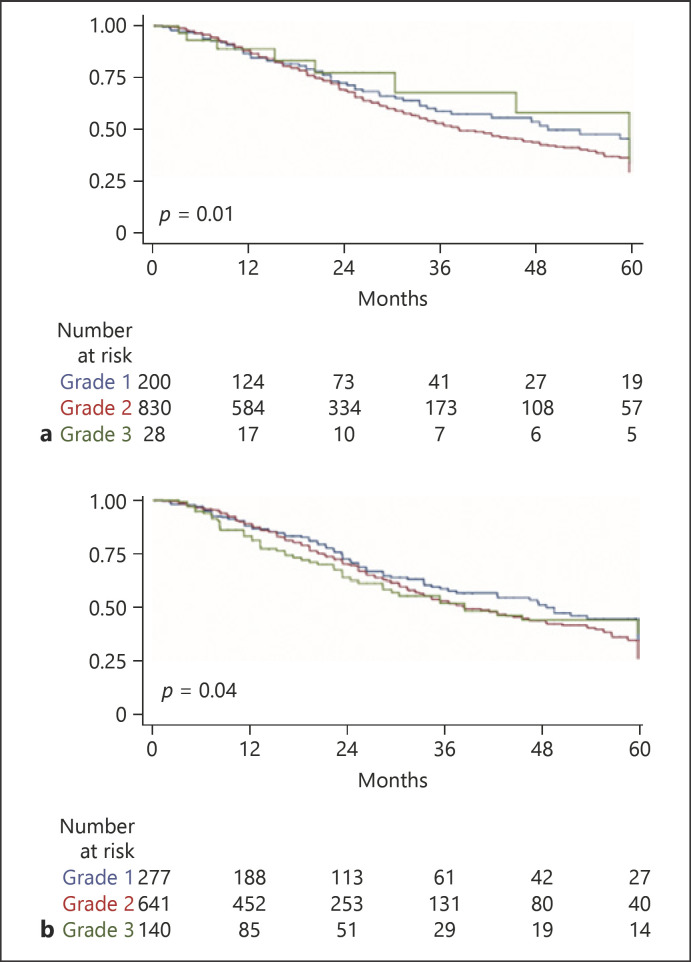
Results: The median OS of the enrolled patients was 41 months. According to LRT χ2 and AIC values based on the time-varying analysis, mHAP-III achieved the best values (41.72 and 4,625.49, respectively, p < 0.0001), indicating the highest predictive performance compared with all other scores (HAP, mHAP-II, ALBI, and pALBI) and staging systems (MELD, ITALICA, CLIP, MESH, MESIAH, JIS, HKLC, and BCLC). In the multivariable Cox proportional hazards model, mHAP-III maintained an independent effect on OS (hazard ratio 1.31, 95% CI: 1.10-1.55, p < 0.0001). Time-varying age, alcoholic etiology, radiologic response to TACE, and performing ablation or surgery after TACE were additional significant variables resulting from the multivariable model.
Conclusion: An innovative time-varying analysis revealed that mHAP-III was the most accurate model in predicting OS in patients with HCC undergoing TACE. Other clinical pre- and post-TACE variables were also found to be relevant for this prediction.
Keywords: ALBI grade; Barcelona Clinic Liver Cancer; Cancer of the Liver Italian Program; ITALICA staging system; MESIAH.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors report the following conflicts of interest related to the present work: Francesco Tovoli: consultant for Bayer and LaForce Guerbet. Fabio Marra: consultant for Bayer, Ipsen, and Eisai and received travel support from Bayer.
Figures
References
-
- Akinyemiju T, Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3((12)):1683–91. - PMC - PubMed
-
- EASL Clinical Practice Guidelines Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. - PubMed
-
- Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 8th ed 2017.
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391((10127)):1301–14. - PubMed
-
- Bolondi L, Burroughs A, Dufour JF, Galle PR, Mazzaferro V, Piscaglia F, et al. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis. 2012;32((4)):348–59. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
