

Characterization of Oligometastatic Disease in a Real-World Nationwide Cohort of 3447 Patients With de Novo Metastatic Breast Cancer
- PMID: 33977227
- PMCID: PMC8099998
- DOI: 10.1093/jncics/pkab010
Characterization of Oligometastatic Disease in a Real-World Nationwide Cohort of 3447 Patients With de Novo Metastatic Breast Cancer
Abstract
Background: Observational studies in metastatic breast cancer (MBC) show that long-term overall survival (OS) is associated with limited tumor burden, or oligo-MBC (OMBC). However, a uniform definition of OMBC is lacking. In this real-world nationwide cohort, we aimed to define the optimal OMBC threshold and factors associated with survival in patients with OMBC.
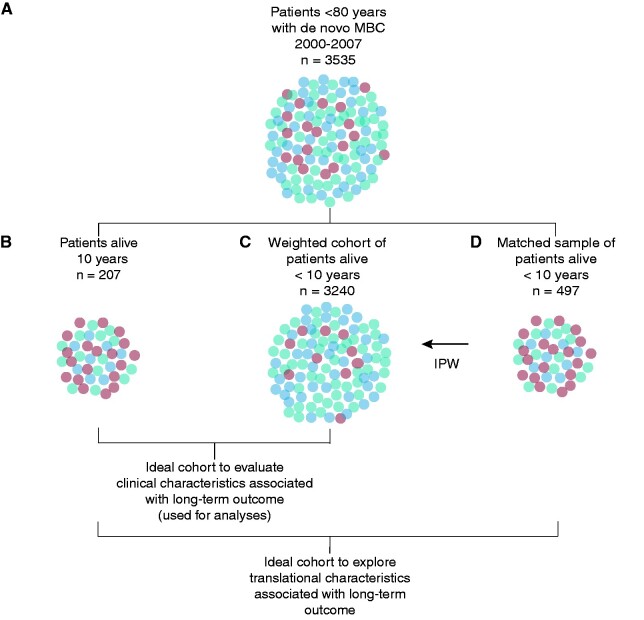
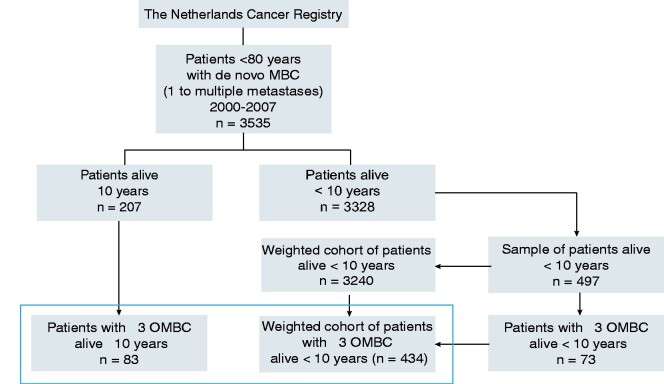
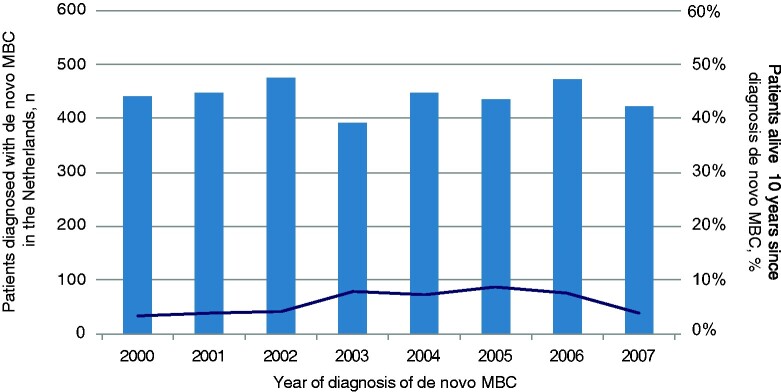
Methods: 3535 patients aged younger than 80 years at diagnosis of de novo MBC in the Netherlands between January 2000 and December 2007 were included. Detailed clinical, therapy, and outcome data were collected from medical records of a sample of the patients. Using inverse-sampling-probability weighting, the analysis cohort (n = 3447) was constructed. We assessed OS according to number of metastases at diagnosis to determine the optimal OMBC threshold. Next, we applied Cox regression models with inverse-sampling-probability weighting to study associations with OS and progression-free survival in OMBC. All statistical tests were 2-sided.
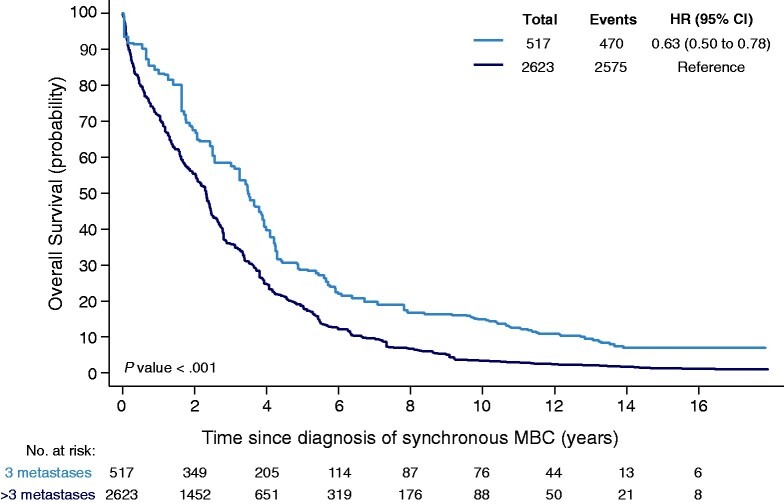
Results: Compared with more than 5 distant metastases, adjusted hazard ratios for OS (with 95% confidence interval [CI] based on robust standard errors) for 1, 2-3, and 4-5 metastases were 0.70 (95% CI = 0.52 to 0.96), 0.63 (95% CI = 0.45 to 0.89), and 0.91 (95% CI = 0.61 to 1.37), respectively. Ten-year OS estimates for patients with no more than 3 vs more than 3 metastases were 14.9% and 3.4% (P < .001). In multivariable analyses, premenopausal andperimenopausal status, absence of lung metastases, and local therapy of metastases (surgery and/or radiotherapy) added to systemic therapy were statistically significantly associated with better OS and progression-free survival in OMBC, independent of local therapy of the primary tumor.
Conclusion: OMBC defined as MBC limited to 1-3 metastases was associated with favorable OS. In OMBC, local therapy of metastases was associated with better OS, particularly if patients were premenopausal or perimenopausal without lung metastases.
© The Author(s) 2021. Published by Oxford University Press.
Figures
Similar articles
-
Characterization of the Tumor Microenvironment of De Novo Oligometastatic Breast Cancer in a Nationwide Cohort.JCO Precis Oncol. 2023 Sep;7:e2200670. doi: 10.1200/PO.22.00670. JCO Precis Oncol. 2023. PMID: 37738542
-
Long-term outcomes of oligometastatic breast cancer patients treated with curative intent: an updated report.Breast Cancer. 2021 Sep;28(5):1051-1061. doi: 10.1007/s12282-021-01240-1. Epub 2021 Apr 11. Breast Cancer. 2021. PMID: 33840010
-
Clinical relevance and low tumor-initiating properties of oligometastatic breast cancer in pulmonary metastasectomy.Breast Cancer Res Treat. 2014 Sep;147(2):317-24. doi: 10.1007/s10549-014-3111-7. Epub 2014 Aug 26. Breast Cancer Res Treat. 2014. PMID: 25156580
-
Possible clinical cure of metastatic breast cancer: lessons from our 30-year experience with oligometastatic breast cancer patients and literature review.Breast Cancer. 2012 Jul;19(3):218-37. doi: 10.1007/s12282-012-0347-0. Epub 2012 Apr 25. Breast Cancer. 2012. PMID: 22532161 Review.
-
Prognostic factors in patients with oligometastatic breast cancer - A systematic review.Cancer Treat Rev. 2020 Dec;91:102114. doi: 10.1016/j.ctrv.2020.102114. Epub 2020 Oct 22. Cancer Treat Rev. 2020. PMID: 33161237
Cited by
-
Oligometastatic breast cancer and metastasis-directed treatment: an aggressive multimodal approach to reach the cure.Ther Adv Med Oncol. 2023 Mar 18;15:17588359231161412. doi: 10.1177/17588359231161412. eCollection 2023. Ther Adv Med Oncol. 2023. PMID: 36950272 Free PMC article. Review.
-
The efficacy of screening with FDG-PET/CT for distant metastases in breast cancer patients scheduled for neoadjuvant systemic therapy.Breast Cancer Res Treat. 2025 Jan;209(1):117-124. doi: 10.1007/s10549-024-07478-5. Epub 2024 Sep 26. Breast Cancer Res Treat. 2025. PMID: 39327358 Free PMC article.
-
St. Gallen/Vienna 2025 Summary of Key Messages on Therapy in Early Breast Cancer from the 2025 St. Gallen International Breast Cancer Conference.Breast Care (Basel). 2025 May 3:1-10. doi: 10.1159/000546080. Online ahead of print. Breast Care (Basel). 2025. PMID: 40546709 Free PMC article. Review.
-
Primary tumor resection in de novo metastatic breast cancer from an oligometastatic perspective: A systematic review and meta-analysis.iScience. 2024 Oct 31;27(12):111224. doi: 10.1016/j.isci.2024.111224. eCollection 2024 Dec 20. iScience. 2024. PMID: 39618499 Free PMC article.
-
Mucin 4 expression is associated with metastasis in triple-negative breast cancer and can be tackled by soluble TNF blockade, improving immunotherapy outcome.Transl Oncol. 2025 Apr;54:102325. doi: 10.1016/j.tranon.2025.102325. Epub 2025 Feb 22. Transl Oncol. 2025. PMID: 39987883 Free PMC article.
References
-
- Palma DA, Salama JK, Lo SS, et al.The oligometastatic state–separating truth from wishful thinking. Nat Rev Clin Oncol. 2014;11(9):549–557. doi: 10.1038/nrclinonc.2014.96 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical