

The value of computed tomography in assessing the risk of death in COVID-19 patients presenting to the emergency room
- PMID: 33978822
- PMCID: PMC8113019
- DOI: 10.1007/s00330-021-07993-9
The value of computed tomography in assessing the risk of death in COVID-19 patients presenting to the emergency room
Abstract
Objective: The aims of this study were to develop a multiparametric prognostic model for death in COVID-19 patients and to assess the incremental value of CT disease extension over clinical parameters.
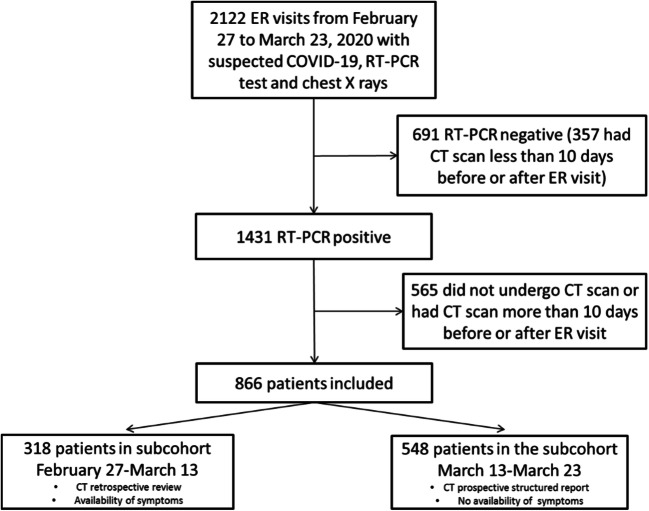
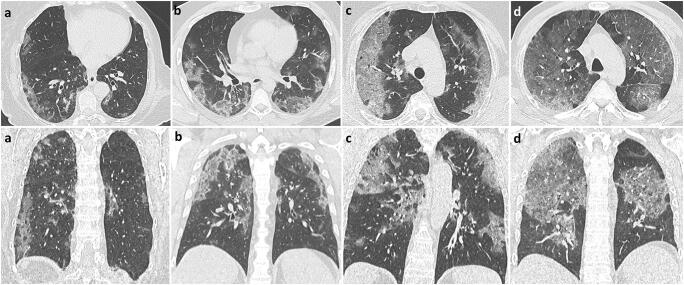
Methods: Consecutive patients who presented to all five of the emergency rooms of the Reggio Emilia province between February 27 and March 23, 2020, for suspected COVID-19, underwent chest CT, and had a positive swab within 10 days were included in this retrospective study. Age, sex, comorbidities, days from symptom onset, and laboratory data were retrieved from institutional information systems. CT disease extension was visually graded as < 20%, 20-39%, 40-59%, or ≥ 60%. The association between clinical and CT variables with death was estimated with univariable and multivariable Cox proportional hazards models; model performance was assessed using k-fold cross-validation for the area under the ROC curve (cvAUC).
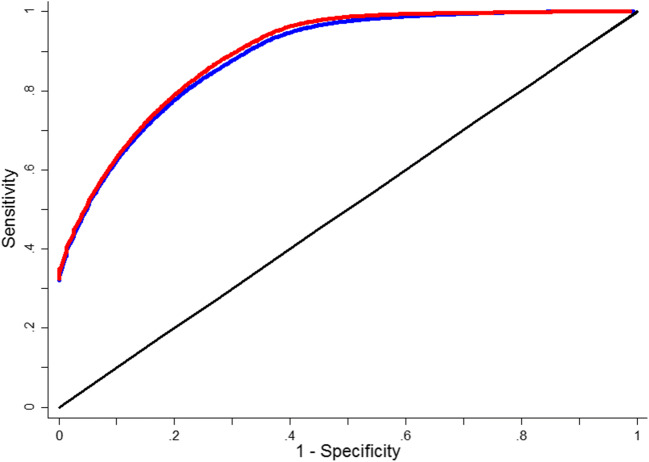
Results: Of the 866 included patients (median age 59.8, women 39.2%), 93 (10.74%) died. Clinical variables significantly associated with death in multivariable model were age, male sex, HDL cholesterol, dementia, heart failure, vascular diseases, time from symptom onset, neutrophils, LDH, and oxygen saturation level. CT disease extension was also independently associated with death (HR = 7.56, 95% CI = 3.49; 16.38 for ≥ 60% extension). cvAUCs were 0.927 (bootstrap bias-corrected 95% CI = 0.899-0.947) for the clinical model and 0.936 (bootstrap bias-corrected 95% CI = 0.912-0.953) when adding CT extension.
Conclusions: A prognostic model based on clinical variables is highly accurate in predicting death in COVID-19 patients. Adding CT disease extension to the model scarcely improves its accuracy.
Key points: • Early identification of COVID-19 patients at higher risk of disease progression and death is crucial; the role of CT scan in defining prognosis is unclear. • A clinical model based on age, sex, comorbidities, days from symptom onset, and laboratory results was highly accurate in predicting death in COVID-19 patients presenting to the emergency room. • Disease extension assessed with CT was independently associated with death when added to the model but did not produce a valuable increase in accuracy.
Keywords: COVID-19; Clinical prediction rule; Multidetector computed tomography; Prognosis.
© 2021. European Society of Radiology.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
