

Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media
- PMID: 33979487
- PMCID: PMC8969083
- DOI: 10.1056/NEJMoa2027278
Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media
Erratum in
-
Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media.N Engl J Med. 2022 May 12;386(19):1868. doi: 10.1056/NEJMx210020. N Engl J Med. 2022. PMID: 35544406 No abstract available.
Abstract
Background: Official recommendations differ regarding tympanostomy-tube placement for children with recurrent acute otitis media.
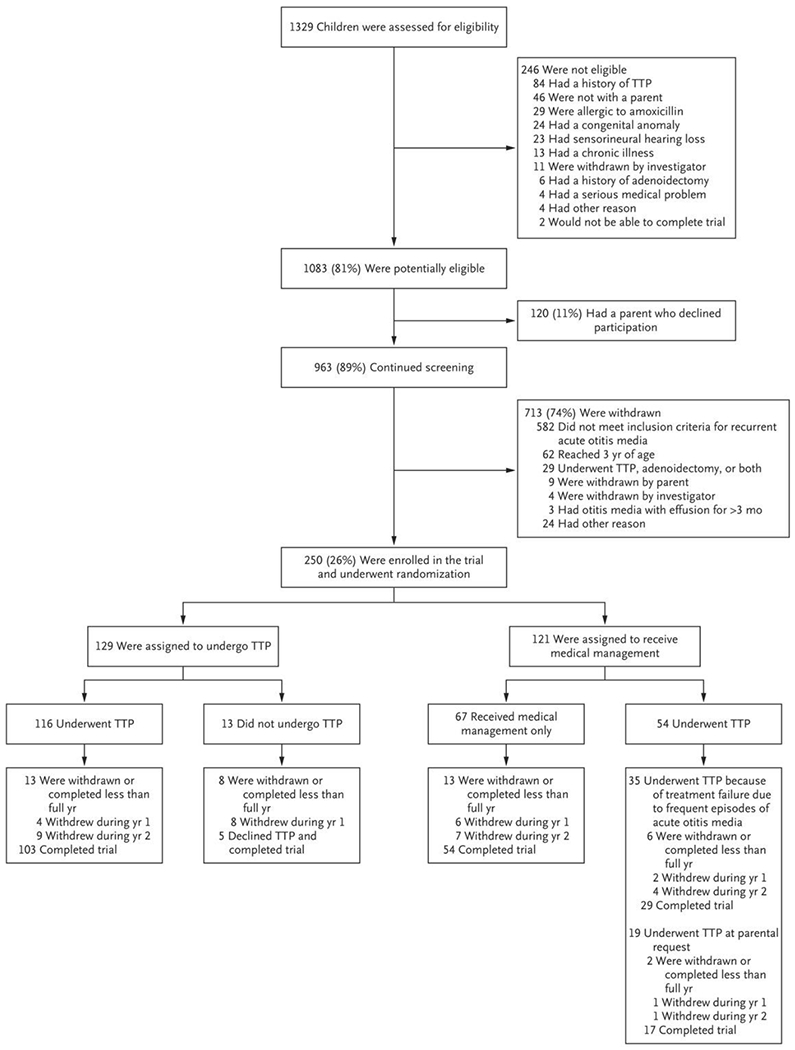
Methods: We randomly assigned children 6 to 35 months of age who had had at least three episodes of acute otitis media within 6 months, or at least four episodes within 12 months with at least one episode within the preceding 6 months, to either undergo tympanostomy-tube placement or receive medical management involving episodic antimicrobial treatment. The primary outcome was the mean number of episodes of acute otitis media per child-year (rate) during a 2-year period.
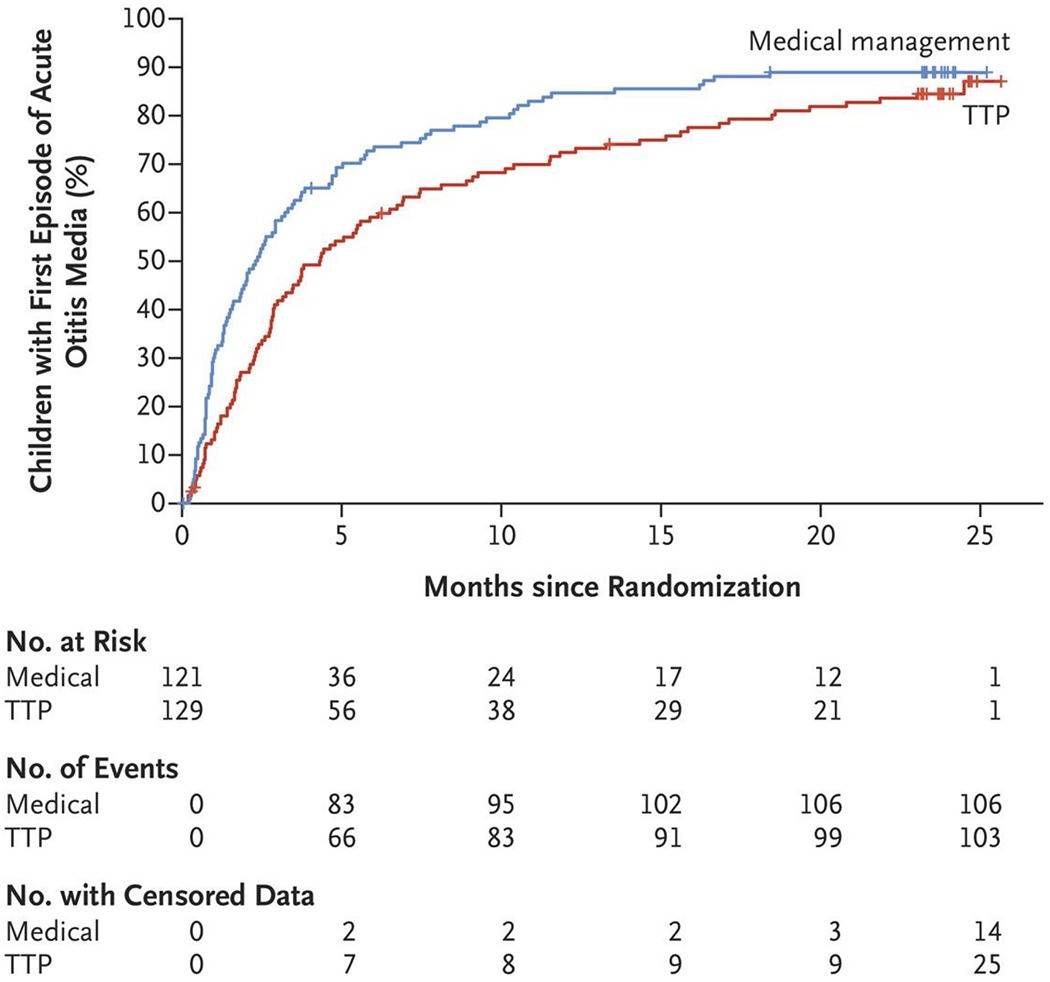
Results: In our main, intention-to-treat analysis, the rate (±SE) of episodes of acute otitis media per child-year during a 2-year period was 1.48±0.08 in the tympanostomy-tube group and 1.56±0.08 in the medical-management group (P = 0.66). Because 10% of the children in the tympanostomy-tube group did not undergo tympanostomy-tube placement and 16% of the children in the medical-management group underwent tympanostomy-tube placement at parental request, we conducted a per-protocol analysis, which gave corresponding episode rates of 1.47±0.08 and 1.72±0.11, respectively. Among secondary outcomes in the main analysis, results were mixed. Favoring tympanostomy-tube placement were the time to a first episode of acute otitis media, various episode-related clinical findings, and the percentage of children meeting specified criteria for treatment failure. Favoring medical management was children's cumulative number of days with otorrhea. Outcomes that did not show substantial differences included the frequency distribution of episodes of acute otitis media, the percentage of episodes considered to be severe, and antimicrobial resistance among respiratory isolates. Trial-related adverse events were limited to those included among the secondary outcomes of the trial.
Conclusions: Among children 6 to 35 months of age with recurrent acute otitis media, the rate of episodes of acute otitis media during a 2-year period was not significantly lower with tympanostomy-tube placement than with medical management. (Funded by the National Institute on Deafness and Other Communication Disorders and others; ClinicalTrials.gov number, NCT02567825.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Management of Recurrent Acute Otitis Media.N Engl J Med. 2021 May 13;384(19):1859-1860. doi: 10.1056/NEJMe2104952. N Engl J Med. 2021. PMID: 33979493 No abstract available.
-
Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media.N Engl J Med. 2021 Aug 26;385(9):860. doi: 10.1056/NEJMc2109725. N Engl J Med. 2021. PMID: 34437790 No abstract available.
-
Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media.N Engl J Med. 2021 Aug 26;385(9):860. doi: 10.1056/NEJMc2109725. N Engl J Med. 2021. PMID: 34437791 No abstract available.
-
Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media.N Engl J Med. 2021 Aug 26;385(9):860-861. doi: 10.1056/NEJMc2109725. N Engl J Med. 2021. PMID: 34437792 No abstract available.
References
-
- Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics 2013;131(3):e964–e999. - PubMed
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Report 2009;(11):1–25. - PubMed
-
- McCann ME, Soriano SG. Does general anesthesia affect neurodevelopment in infants and children? BMJ 2019;367:l6459. - PubMed
-
- Ah-Tye C, Paradise JL, Colborn DK. Otorrhea in young children after tympanostomy-tube placement for persistent middle-ear effusion: prevalence, incidence, and duration. Pediatrics 2001;107:1251–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical