

Thorny ground, rocky soil: Tissue-specific mechanisms of tumor dormancy and relapse
- PMID: 33979673
- PMCID: PMC9595433
- DOI: 10.1016/j.semcancer.2021.05.007
Thorny ground, rocky soil: Tissue-specific mechanisms of tumor dormancy and relapse
Abstract
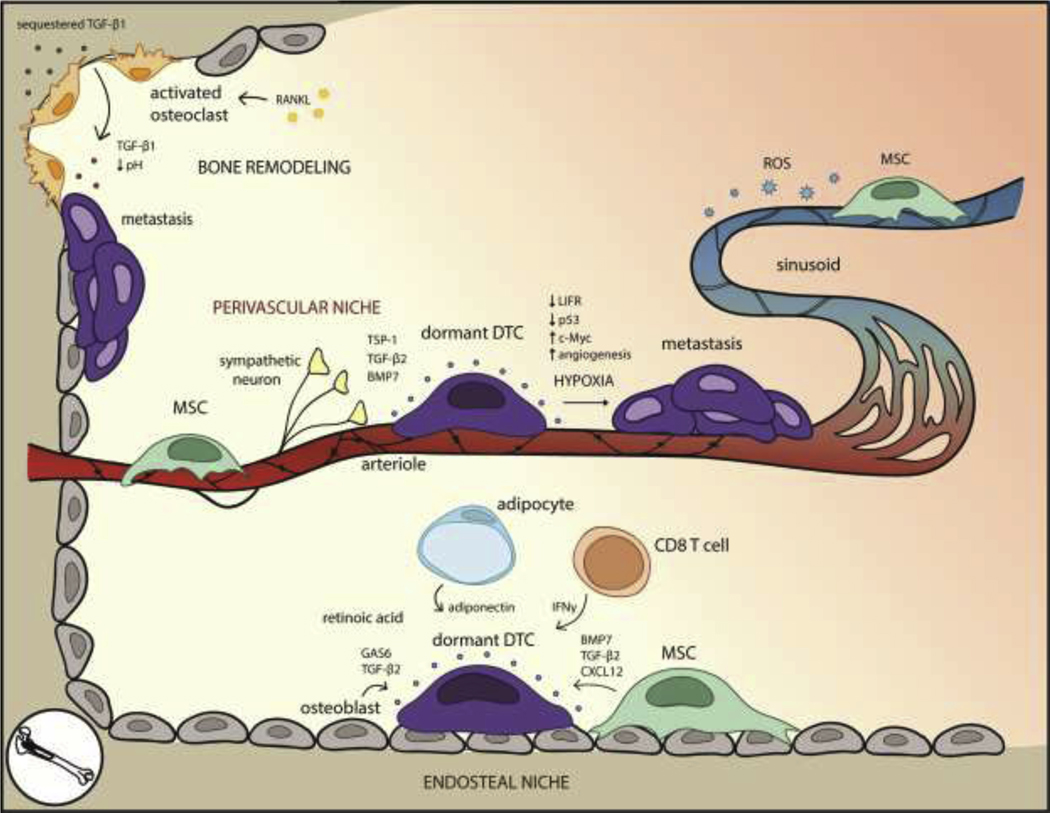
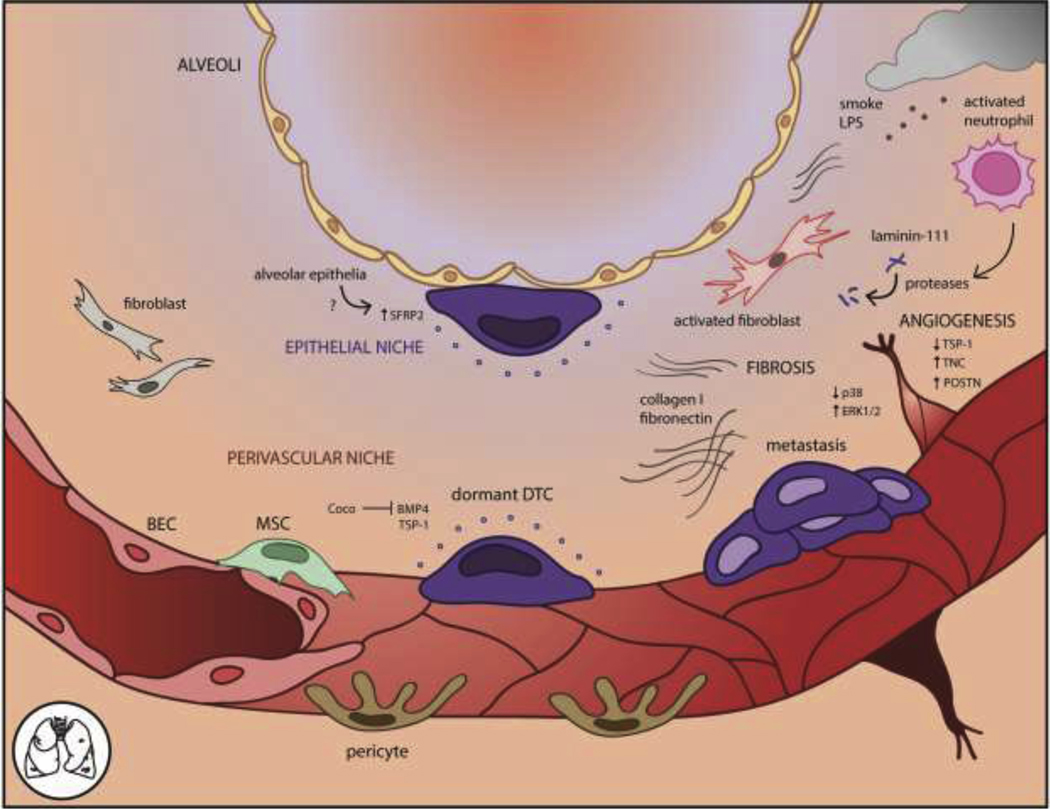
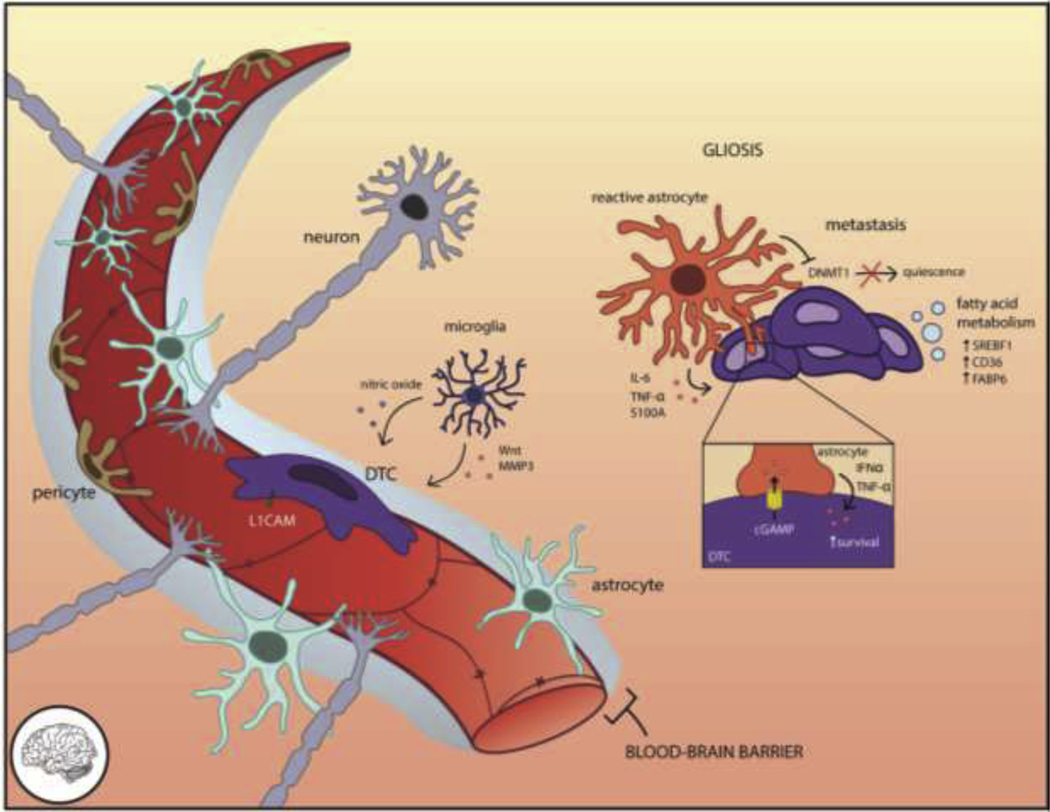
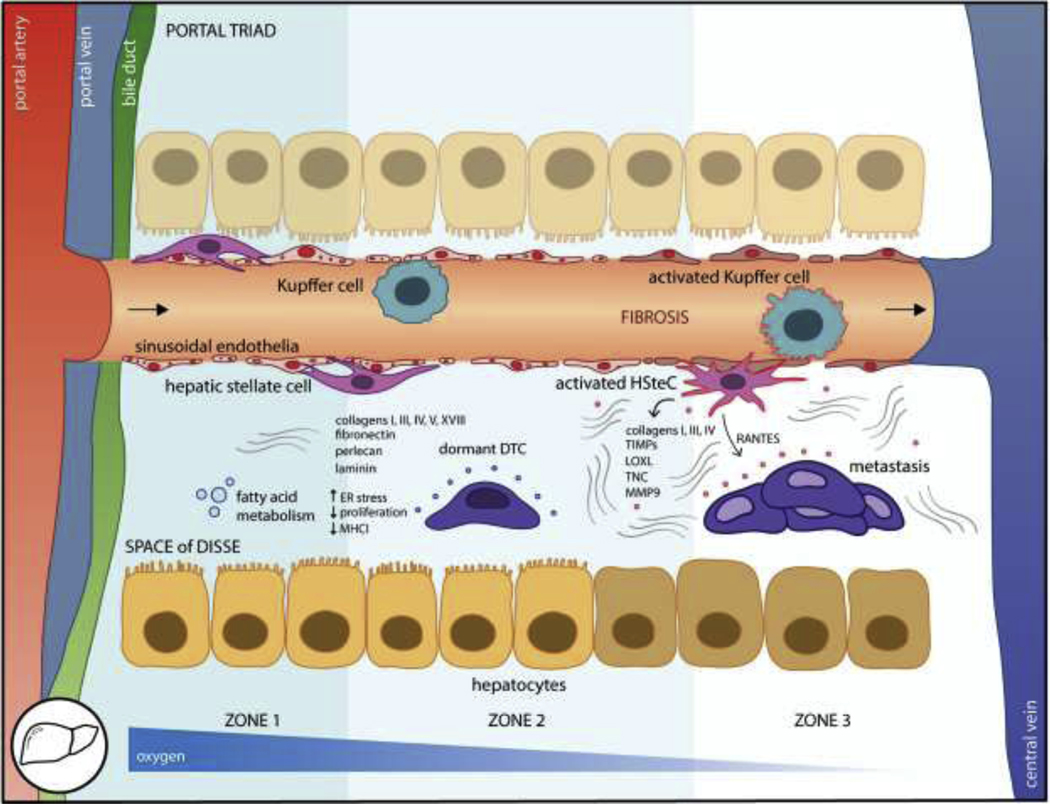
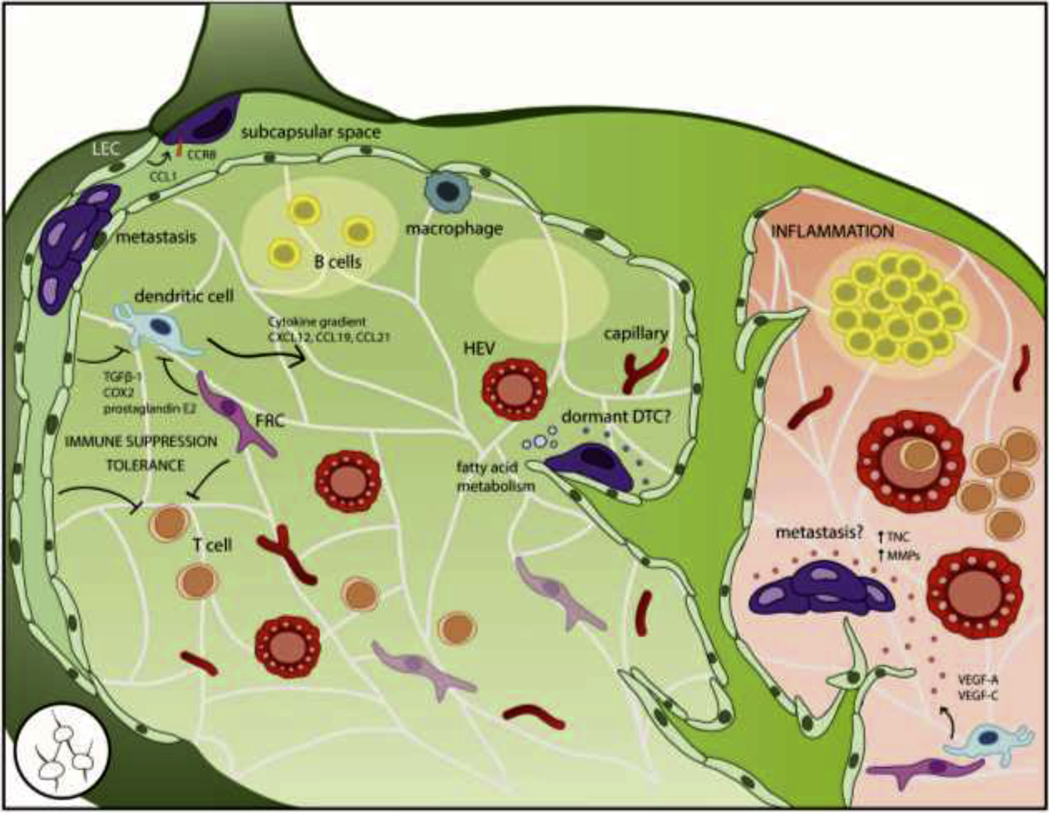
Disseminated tumor cells (DTCs) spread systemically yet distinct patterns of metastasis indicate a range of tissue susceptibility to metastatic colonization. Distinctions between permissive and suppressive tissues are still being elucidated at cellular and molecular levels. Although there is a growing appreciation for the role of the microenvironment in regulating metastatic success, we have a limited understanding of how diverse tissues regulate DTC dormancy, the state of reversible quiescence and subsequent awakening thought to contribute to delayed relapse. Several themes of microenvironmental regulation of dormancy are beginning to emerge, including vascular association, co-option of pre-existing niches, metabolic adaptation, and immune evasion, with tissue-specific nuances. Conversely, DTC awakening is often associated with injury or inflammation-induced activation of the stroma, promoting a proliferative environment with DTCs following suit. We review what is known about tissue-specific regulation of tumor dormancy on a tissue-by-tissue basis, profiling major metastatic organs including the bone, lung, brain, liver, and lymph node. An aerial view of the barriers to metastatic growth may reveal common targets and dependencies to inform the therapeutic prevention of relapse.
Keywords: Disseminated tumor cell dormancy; Dormant niche; Metastasis; Microenvironment; Quiescence.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest statement
The authors declare that there are no conflicts of interest.
Figures
References
-
- Spencer W, Celsus de Medicina. The American Journal of the Medical Sciences, 1936. 191(3): p. 424.
-
- Lluch A, et al., Dynamic clonal remodelling in breast cancer metastases is associated with subtype conversion. European Journal of Cancer, 2019. 120: p. 54–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
