

Access to Mechanical Thrombectomy for Ischemic Stroke in the United States
- PMID: 33980045
- PMCID: PMC8316281
- DOI: 10.1161/STROKEAHA.120.033485
Access to Mechanical Thrombectomy for Ischemic Stroke in the United States
Abstract
Background and purpose: Mechanical thrombectomy helps prevent disability in patients with acute ischemic stroke involving occlusion of a large cerebral vessel. Thrombectomy requires procedural expertise and not all hospitals have the staff to perform this intervention. Few population-wide data exist regarding access to mechanical thrombectomy.
Methods: We examined access to thrombectomy for ischemic stroke using discharge data from calendar years 2016 to 2018 from all nonfederal emergency departments and acute care hospitals across 11 US states encompassing 80 million residents. Facilities were classified as hubs if they performed mechanical thrombectomy, gateways if they transferred patients who ultimately underwent mechanical thrombectomy, and gaps otherwise. We used standard descriptive statistics and unadjusted logistic regression models in our primary analyses.
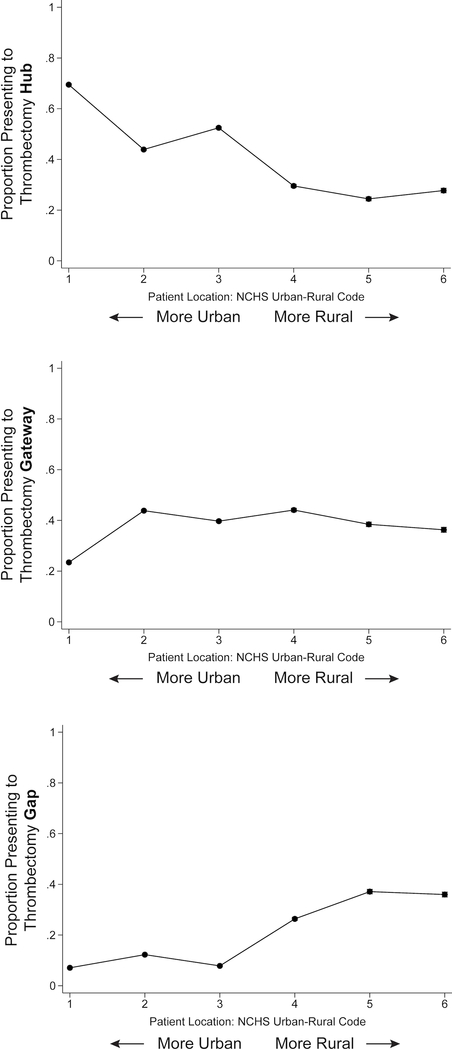
Results: Among 205 681 patients with ischemic stroke, 100 139 (48.7% [95% CI, 48.5%–48.9%]) initially received care at a thrombectomy hub, 72 534 (35.3% [95% CI, 35.1%–35.5%]) at a thrombectomy gateway, and 33 008 (16.0% [95% CI, 15.9%–16.2%]) at a thrombectomy gap. Patients who initially received care at thrombectomy gateways were substantially less likely to ultimately undergo thrombectomy than patients who initially received care at thrombectomy hubs (odds ratio, 0.27 [95% CI, 0.25–0.28]). Rural patients had particularly limited access: 27.7% (95% CI, 26.9%–28.6%) of such patients initially received care at hubs versus 69.5% (95% CI, 69.1%–69.9%) of urban patients. For 93.8% (95% CI, 93.6%–94.0%) of patients with stroke at gateways, their initial facility was capable of delivering intravenous thrombolysis, compared with 76.3% (95% CI, 75.8%–76.7%) of patients at gaps. Our findings were unchanged in models adjusted for demographics and comorbidities and persisted across multiple sensitivity analyses, including analyses adjusting for estimated stroke severity.
Conclusions: We found that a substantial proportion of patients with ischemic stroke across the United States lacked access to thrombectomy even after accounting for interhospital transfers. US systems of stroke care require further development to optimize thrombectomy access.
Keywords: United States; access to treatment; healthcare systems; ischemic stroke; thrombectomy.
Figures
 81% - 100%
81% - 100%  61% - 80%
61% - 80%  41% - 60%
41% - 60%  21% - 40%
21% - 40%  0% - 20%
0% - 20% 81% - 100% 61% - 80% 41% - 60% 21% - 40% 0% - 20%
81% - 100% 61% - 80% 41% - 60% 21% - 40% 0% - 20%References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DWJ, Mitchell PJ, Demchuk AM, Dávalos A, Majoie CBLM, van der Lugt A, de Miquel MA, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. The Lancet. 2016;387:1723–1731. - PubMed
-
- Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, Johnston KC, Johnston SC, Khalessi AA, Kidwell CS, et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46:3020–3035. - PubMed
-
- Jahan R, Saver JL, Schwamm LH, Fonarow GC, Liang L, Matsouaka RA, Xian Y, Holmes DN, Peterson ED, Yavagal D, et al. Association Between Time to Treatment With Endovascular Reperfusion Therapy and Outcomes in Patients With Acute Ischemic Stroke Treated in Clinical Practice. JAMA. 2019;322:252–263. - PMC - PubMed
-
- Kunz WG, Hunink MG, Almekhlafi MA, Menon BK, Saver JL, Dippel DWJ, Majoie C, Jovin TG, Davalos A, Bracard S, et al. Public health and cost consequences of time delays to thrombectomy for acute ischemic stroke. Neurology. 2020;95:e2465–e2475. - PubMed
-
- Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality. https://www.hcup-us.ahrq.gov. Accessed February 13, 2020. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
