

A case report of individualized ventilation in a COVID-19 patient - new possibilities and caveats to consider with flow-controlled ventilation
- PMID: 33980178
- PMCID: PMC8113787
- DOI: 10.1186/s12871-021-01365-y
A case report of individualized ventilation in a COVID-19 patient - new possibilities and caveats to consider with flow-controlled ventilation
Abstract
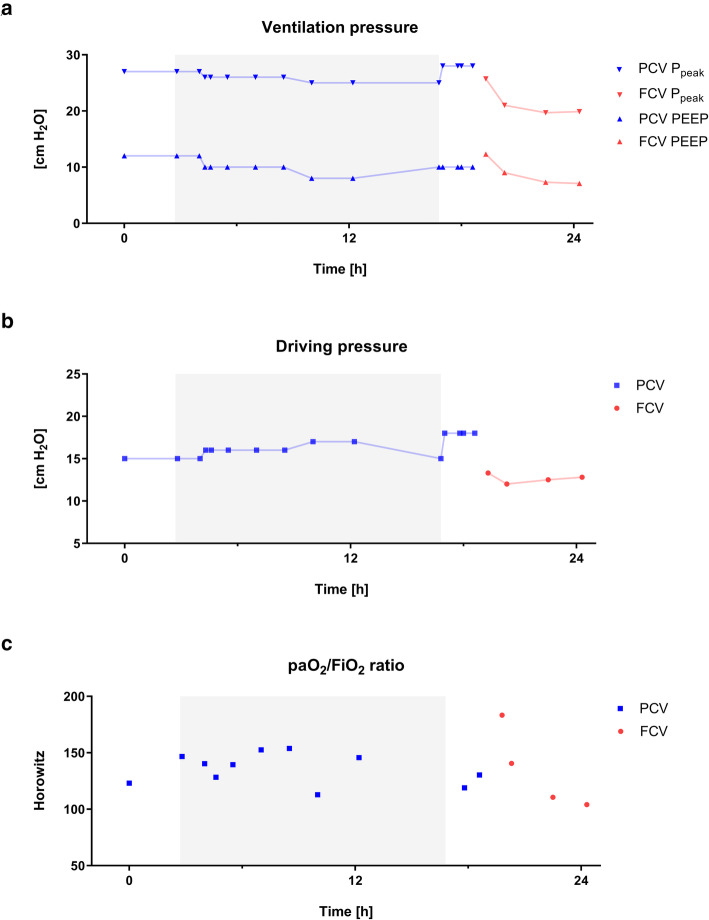
Background: Flow-controlled ventilation (FCV) is a novel ventilation method increasingly being used clinically, particularly during the current COVID-19 pandemic. However, the continuous flow pattern in FCV during inspiration and expiration has a significant impact on respiratory parameters and ventilatory settings compared to conventional ventilation modes. In addition, the constant flow combined with direct intratracheal pressure measurement allows determination of dynamic compliance and ventilation settings can be adjusted accordingly, reflecting a personalized ventilation approach.
Case presentation: A 50-year old women with confirmed SARS-CoV-2 infection suffering from acute respiratory distress syndrome (ARDS) was admitted to a tertiary medical center. Initial ventilation occurred with best standard of care pressure-controlled ventilation (PCV) and was then switched to FCV, by adopting PCV ventilator settings. This led to an increase in oxygenation by 30 %. Subsequently, to reduce invasiveness of mechanical ventilation, FCV was individualized by dynamic compliance guided adjustment of both, positive end-expiratory pressure and peak pressure; this intervention reduced driving pressure from 18 to 12 cm H2O. However, after several hours, compliance further deteriorated which resulted in a tidal volume of only 4.7 ml/kg.
Conclusions: An individualized FCV approach increased oxygenation parameters in a patient suffering from severe COVID-19 related ARDS. Direct intratracheal pressure measurements allow for determination of dynamic compliance and thus optimization of ventilator settings, thereby reducing applied and dissipated energy. However, although desirable, this personalized ventilation strategy may reach its limits when lung function is so severely impaired that patient's oxygenation has to be ensured at the expense of lung protective ventilation concepts.
Keywords: COVID-19; Case Report; Lung Compliance; Respiratory Distress Syndrome, Adult; Stress Mechanical.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- ARDS Definition Task Force. Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: The berlin definition. JAMA. 2012;307(23):2526–33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
