

Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies
- PMID: 33980222
- PMCID: PMC8117497
- DOI: 10.1186/s12916-021-01978-7
Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies
Erratum in
-
Correction to: Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies.BMC Med. 2021 Sep 8;19(1):228. doi: 10.1186/s12916-021-02112-3. BMC Med. 2021. PMID: 34496860 Free PMC article. No abstract available.
Abstract
Background: Improved access to effective antiretroviral therapy has meant that people living with HIV (PLHIV) are surviving to older ages. However, PLHIV may be ageing differently to HIV-negative individuals, with dissimilar burdens of non-communicable diseases, such as hypertension. While some observational studies have reported a higher risk of prevalent hypertension among PLHIV compared to HIV-negative individuals, others have found a reduced burden. To clarify the relationship between HIV and hypertension, we identified observational studies and pooled their results to assess whether there is a difference in hypertension risk by HIV status.
Methods: We performed a global systematic review and meta-analysis of published cross-sectional studies that examined hypertension risk by HIV status among adults aged > 15 (PROSPERO: CRD42019151359). We searched MEDLINE, EMBASE, Global Health and Cochrane CENTRAL to August 23, 2020, and checked reference lists of included articles. Our main outcome was the risk ratio for prevalent hypertension in PLHIV compared to HIV-negative individuals. Summary estimates were pooled with a random effects model and meta-regression explored whether any difference was associated with study-level factors.
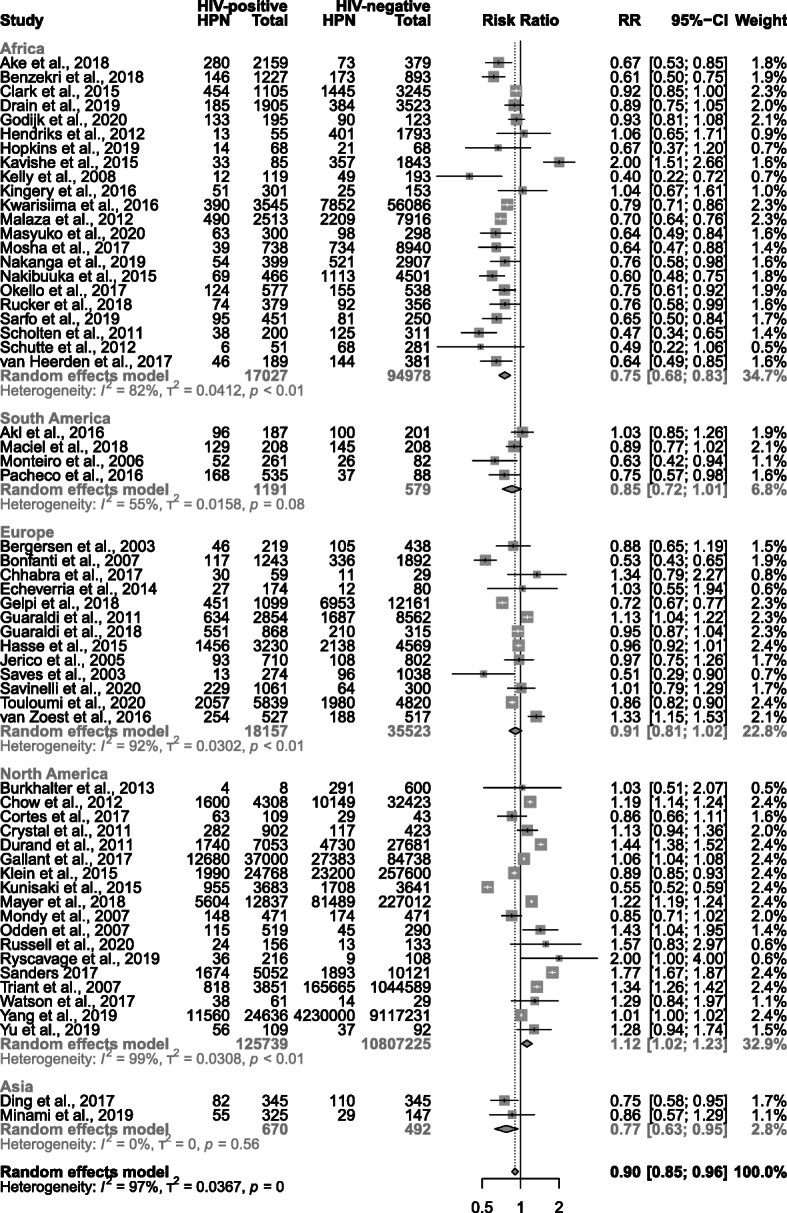
Results: Of 21,527 identified studies, 59 were eligible (11,101,581 participants). Crude global hypertension risk was lower among PLHIV than HIV-negative individuals (risk ratio 0.90, 95% CI 0.85-0.96), although heterogeneity between studies was high (I2 = 97%, p < 0.0001). The relationship varied by continent, with risk higher among PLHIV in North America (1.12, 1.02-1.23) and lower among PLHIV in Africa (0.75, 0.68-0.83) and Asia (0.77, 0.63-0.95). Meta-regression revealed strong evidence of a difference in risk ratios when comparing North American and European studies to African ones (North America 1.45, 1.21-1.74; Europe 1.20, 1.03-1.40).
Conclusions: Our findings suggest that the relationship between HIV status and prevalent hypertension differs by region. The results highlight the need to tailor hypertension prevention and care to local contexts and underscore the importance of rapidly optimising integration of services for HIV and hypertension in the worst affected regions. The role of different risk factors for hypertension in driving context-specific trends remains unclear, so development of further cohorts of PLHIV and HIV-negative controls focused on this would also be valuable.
Keywords: Blood pressure; HIV; Hypertension; Meta-analysis; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Marcus JL, Leyden WA, Alexeeff SE, Anderson AN, Hechter RC, Hu H, Lam JO, Towner WJ, Yuan Q, Horberg MA, Silverberg MJ. Comparison of overall and comorbidity-free life expectancy between insured adults with and without HIV infection, 2000-2016. JAMA Netw Open. 2020;3(6):e207954. doi: 10.1001/jamanetworkopen.2020.7954. - DOI - PMC - PubMed
-
- Mayer KH, Loo S, Crawford PM, Crane HM, Leo M, DenOuden P, Houlberg M, Schmidt M, Quach T, Ruhs S, Vandermeer M, Grasso C, McBurnie MA. Excess clinical comorbidity among HIV-infected patients accessing primary care in US community health centers. Public Health Rep. 2018;133(1):109–118. doi: 10.1177/0033354917748670. - DOI - PMC - PubMed
-
- van Zoest RA, Wit FW, Kooij KW, van der Valk M, Schouten J, Kootstra NA, Wiersinga WJ, Prins M, van den Born B, Reiss P, AGEhIV Cohort Study Group Higher prevalence of hypertension in HIV-1-infected patients on combination antiretroviral therapy is associated with changes in body composition and prior Stavudine exposure. Clin Infect Dis. 2016;63(2):205–213. doi: 10.1093/cid/ciw285. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
