

False lumen pressure estimation in type B aortic dissection using 4D flow cardiovascular magnetic resonance: comparisons with aortic growth
- PMID: 33980249
- PMCID: PMC8117268
- DOI: 10.1186/s12968-021-00741-4
False lumen pressure estimation in type B aortic dissection using 4D flow cardiovascular magnetic resonance: comparisons with aortic growth
Abstract
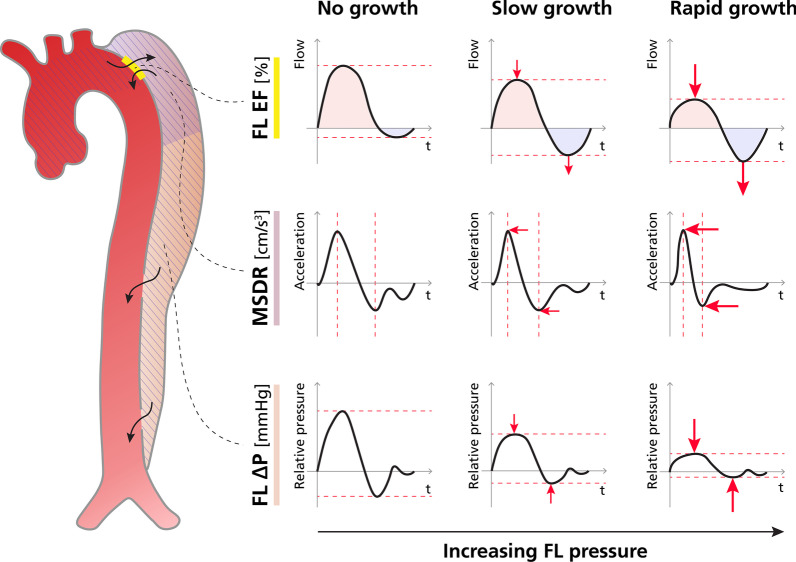
Background: Chronic type B aortic dissection (TBAD) is associated with poor long-term outcome, and accurate risk stratification tools remain lacking. Pressurization of the false lumen (FL) has been recognized as central in promoting aortic growth. Several surrogate imaging-based metrics have been proposed to assess FL hemodynamics; however, their relationship to enlarging aortic dimensions remains unclear. We investigated the association between aortic growth and three cardiovascular magnetic resonance (CMR)-derived metrics of FL pressurization: false lumen ejection fraction (FLEF), maximum systolic deceleration rate (MSDR), and FL relative pressure (FL ΔPmax).
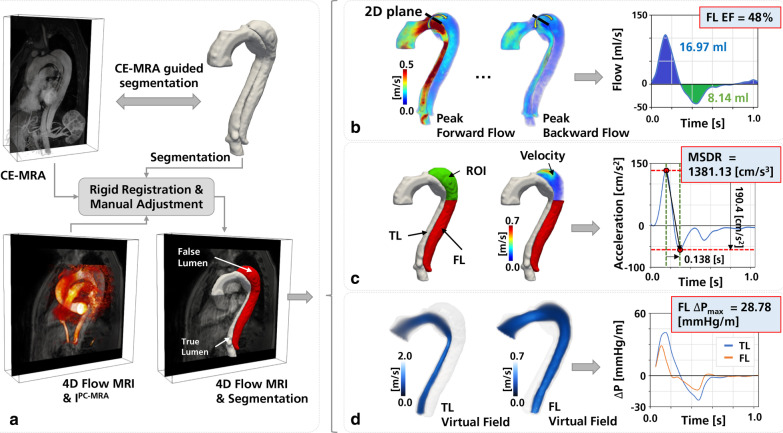
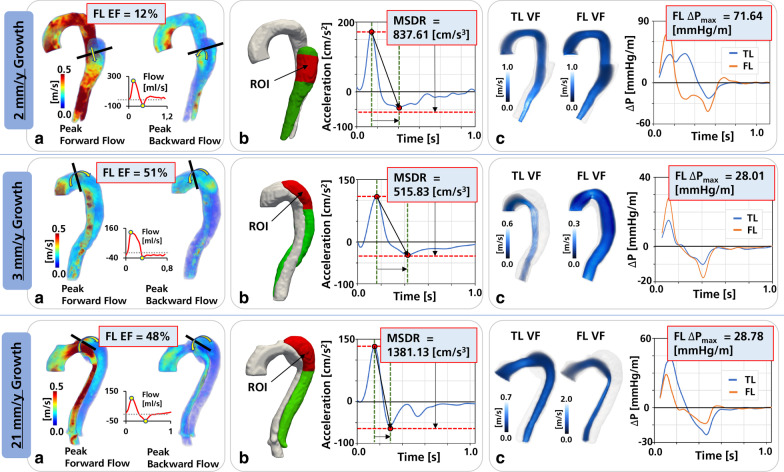
Methods: CMR/CMR angiography was performed in 12 patients with chronic dissection of the descending thoracoabdominal aorta, including contrast-enhanced CMR angiography and time-resolved three-dimensional phase-contrast CMR (4D Flow CMR). Aortic growth rate was calculated as the change in maximal aortic diameter between baseline and follow-up imaging studies over the time interval, with patients categorized as having either 'stable' (< 3 mm/year) or 'enlarging' (≥ 3 mm/year) growth. Three metrics relating to FL pressurization were defined as: (1) FLEF: the ratio between retrograde and antegrade flow at the TBAD entry tear, (2) MSDR: the absolute difference between maximum and minimum systolic acceleration in the proximal FL, and (3) FL ΔPmax: the difference in absolute pressure between aortic root and distal FL.
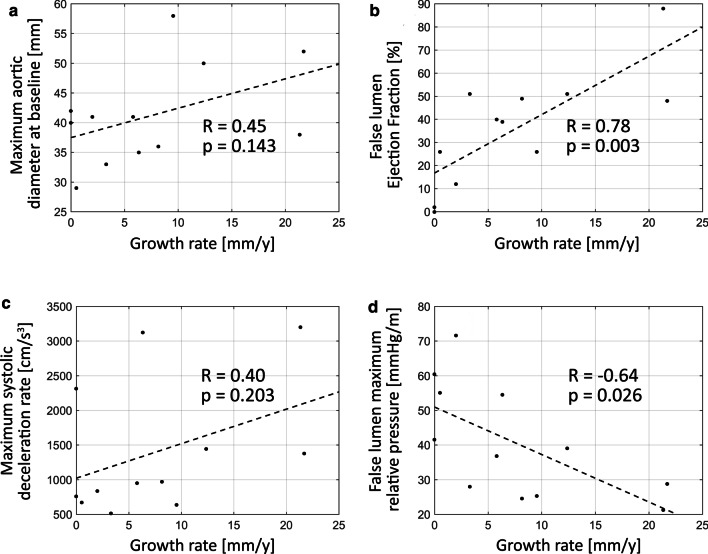
Results: FLEF was higher in enlarging TBAD (49.0 ± 17.9% vs. 10.0 ± 11.9%, p = 0.002), whereas FL ΔPmax was lower (32.2 ± 10.8 vs. 57.2 ± 12.5 mmHg/m, p = 0.017). MSDR and conventional anatomic variables did not differ significantly between groups. FLEF showed positive (r = 0.78, p = 0.003) correlation with aortic growth rate whereas FL ΔPmax showed negative correlation (r = - 0.64, p = 0.026). FLEF and FL ΔPmax remained as independent predictors of aortic growth rate after adjusting for baseline aortic diameter.
Conclusion: Comparative analysis of three 4D flow CMR metrics of TBAD FL pressurization demonstrated that those that focusing on retrograde flow (FLEF) and relative pressure (FL ΔPmax) independently correlated with growth and differentiated patients with enlarging and stable descending aortic dissections. These results emphasize the highly variable nature of aortic hemodynamics in TBAD patients, and suggest that 4D Flow CMR derived metrics of FL pressurization may be useful to separate patients at highest and lowest risk for progressive aortic growth and complications.
Keywords: 4D flow MRI; 4D flow magnetic resonance imaging; Aortic growth rate; False lumen; False lumen ejection fraction; Maximum systolic deceleration rate; Relative pressure; Type B aortic dissection.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Interval changes in four-dimensional flow-derived in vivo hemodynamics stratify aortic growth in type B aortic dissection patients.J Cardiovasc Magn Reson. 2024 Winter;26(2):101078. doi: 10.1016/j.jocmr.2024.101078. Epub 2024 Aug 2. J Cardiovasc Magn Reson. 2024. PMID: 39098572 Free PMC article.
-
False lumen ejection fraction predicts growth in type B aortic dissection: preliminary results.Eur J Cardiothorac Surg. 2020 May 1;57(5):896-903. doi: 10.1093/ejcts/ezz343. Eur J Cardiothorac Surg. 2020. PMID: 31821480 Free PMC article.
-
False lumen hemodynamics and partial thrombosis in chronic aortic dissection of the descending aorta.Eur Radiol. 2024 Aug;34(8):5190-5200. doi: 10.1007/s00330-023-10513-6. Epub 2024 Jan 6. Eur Radiol. 2024. PMID: 38183450
-
Fate and Consequences of the False Lumen After Thoracic Endovascular Aortic Repair in Type B Aortic Dissection.Ann Vasc Surg. 2023 Aug;94:32-37. doi: 10.1016/j.avsg.2022.09.042. Epub 2022 Oct 26. Ann Vasc Surg. 2023. PMID: 36309167 Review.
-
In Vitro Studies on Hemodynamics of Type B Aortic Dissection: Accuracy and Reliability.J Endovasc Ther. 2025 Apr;32(2):303-311. doi: 10.1177/15266028231182229. Epub 2023 Jun 21. J Endovasc Ther. 2025. PMID: 37341214 Review.
Cited by
-
Clinical Imaging and Innovations in Aortic Aneurysm and Dissection.Semin Intervent Radiol. 2024 Dec 9;41(6):536-546. doi: 10.1055/s-0044-1800823. eCollection 2024 Dec. Semin Intervent Radiol. 2024. PMID: 40190769 Review.
-
Observation of intracranial artery and venous sinus hemodynamics using compressed sensing-accelerated 4D flow MRI: performance at different acceleration factors.Front Neurosci. 2024 Jul 25;18:1438003. doi: 10.3389/fnins.2024.1438003. eCollection 2024. Front Neurosci. 2024. PMID: 39119457 Free PMC article.
-
Mechanisms of aortic dissection: From pathological changes to experimental and in silico models.Prog Mater Sci. 2025 Apr;150:101363. doi: 10.1016/j.pmatsci.2024.101363. Epub 2024 Sep 12. Prog Mater Sci. 2025. PMID: 39830801 Free PMC article.
-
Interval changes in four-dimensional flow-derived in vivo hemodynamics stratify aortic growth in type B aortic dissection patients.J Cardiovasc Magn Reson. 2024 Winter;26(2):101078. doi: 10.1016/j.jocmr.2024.101078. Epub 2024 Aug 2. J Cardiovasc Magn Reson. 2024. PMID: 39098572 Free PMC article.
-
Baseline 4D Flow-Derived in vivo Hemodynamic Parameters Stratify Descending Aortic Dissection Patients With Enlarging Aortas.Front Cardiovasc Med. 2022 Jun 9;9:905718. doi: 10.3389/fcvm.2022.905718. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35757320 Free PMC article.
References
-
- Tsai TT, Evangelista A, Nienaber CA, Trimarchi S, Sechtem U, Fattori R, et al. Long-term survival in patients presenting with type A acute aortic dissection: insights from the International Registry of Acute Aortic Dissection (IRAD) Circulation. 2006;114(1_supplement):I-350–I-356. - PubMed
-
- Nienaber CA, Kische S, Rousseau H, Eggebrecht H, Rehders TC, Kundt G, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6(4):407–416. doi: 10.1161/CIRCINTERVENTIONS.113.000463. - DOI - PubMed
-
- Fattori R, Montgomery D, Lovato L, Kische S, Di Eusanio M, Ince H, et al. Survival after endovascular therapy in patients with type B aortic dissection: a report from the International Registry of Acute Aortic Dissection (IRAD) JACC Cardiovasc Interv. 2013;6(8):876–882. doi: 10.1016/j.jcin.2013.05.003. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
