

Patient-specific instrumentation combined with a new tool for gap balancing is useful in total knee replacement: a 3-year follow-up of a retrospective study
- PMID: 33980282
- PMCID: PMC8114523
- DOI: 10.1186/s13018-021-02467-6
Patient-specific instrumentation combined with a new tool for gap balancing is useful in total knee replacement: a 3-year follow-up of a retrospective study
Abstract
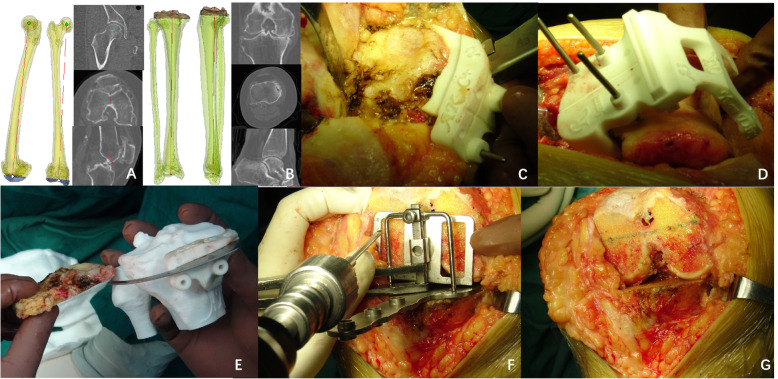
Objective: The purpose of this study was to determine whether the gap-balancing technique with patient-specific instrumentation (PSI) and a new balancing device in total knee arthroplasty (TKA) can improve knee function to a greater extent than can the measured resection technique.
Materials and methods: Data from 150 patients who underwent TKA from August 2014 to June 2016 were studied retrospectively. The gap-balancing technique assisted by PSI and the new balancing device was used in 80 patients (82 knees), and the measured resection technique was used in 70 patients (70 knees). The surgical, imaging, and knee function data were compared.
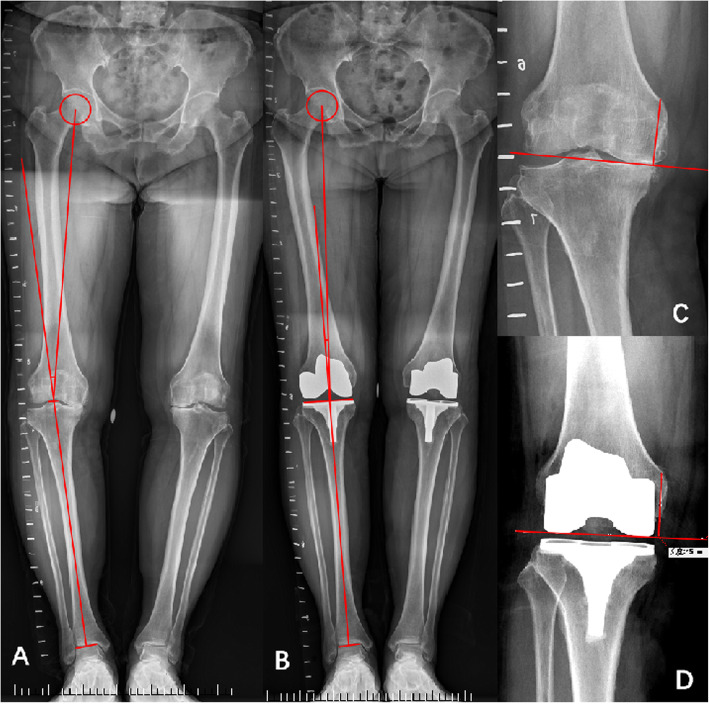
Results: The gap-balancing technique assisted by PSI and the new balancing device was found to be feasible in all operated knees and reliable. In total, 150 patients (152 knees) of ages ranging from 52 to 78 years (mean 67 years) underwent TKA during the study period. The follow-up period ranged from 35 to 52 months (mean 45 months). Only one patient, who was included in the gap-balancing group, underwent a revision surgery at 2 years postoperatively due to infection. There were no differences in the incidence of anterior knee pain between the two groups. The mean flexion angle, KSS scores, and VAS scores did not significantly differ between the measured resection group and gap-balancing group at 12 weeks or 36 weeks postoperatively. The average joint line displacement was 1.3 ± 1.1 mm (range 0-3) proximally in the GB (gap-balancing) group and 1.2 ± 1.4 mm in the MR (measured-resection) group. No outliers >5 mm in either group were recorded. The mean leg axis deviation from the neutral mechanical axis was 1.8°±1.5° varus (range 0°-3°varus) versus the neutral mechanical axis in the GB group and 1.4°±1.2°(range 0°-3°)in the MR group. No outliers with >3° deviation in either group were recorded.
Conclusions: The gap-balancing technique performed with the new balancing device and PSI can yield accurate femoral component alignment as well as outcomes similar to those of measured resection at 3 years. The new balancing device can be taken into consideration by surgeons who prefer performing the gap-balancing technique with PSI.
Keywords: Balancer device; Equipment design; Flexion-extension gap surgical technique; Gap balance; Implantation technique; Ligament balance; Measured resection technique; Total knee arthroplasty.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Spacer-based gap balancing is useful in total knee arthroplasty: a 3-year follow-up of a retrospective study.J Orthop Surg Res. 2021 Oct 21;16(1):633. doi: 10.1186/s13018-021-02788-6. J Orthop Surg Res. 2021. PMID: 34674736 Free PMC article.
-
Gap-balancing technique combined with patient-specific instrumentation in TKA.Arch Orthop Trauma Surg. 2015 Nov;135(11):1603-8. doi: 10.1007/s00402-015-2315-6. Epub 2015 Aug 28. Arch Orthop Trauma Surg. 2015. PMID: 26315332
-
What Factors Are Associated With Femoral Component Internal Rotation in TKA Using the Gap Balancing Technique?Clin Orthop Relat Res. 2017 Aug;475(8):1999-2010. doi: 10.1007/s11999-017-5319-4. Epub 2017 Mar 23. Clin Orthop Relat Res. 2017. PMID: 28337656 Free PMC article.
-
Comparison of soft tissue balancing, femoral component rotation, and joint line change between the gap balancing and measured resection techniques in primary total knee arthroplasty: A meta-analysis.Medicine (Baltimore). 2016 Sep;95(39):e5006. doi: 10.1097/MD.0000000000005006. Medicine (Baltimore). 2016. PMID: 27684862 Free PMC article. Review.
-
Clinical Outcomes of Gap Balancing vs Measured Resection in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis Involving 2259 Subjects.J Arthroplasty. 2018 Aug;33(8):2684-2693. doi: 10.1016/j.arth.2018.03.015. Epub 2018 Mar 17. J Arthroplasty. 2018. PMID: 29656972
Cited by
-
Making a Joint Decision Regarding the Timing of Surgery for Elective Arthroplasty Surgery After Being Infected With COVID-19: A Systematic Review.J Arthroplasty. 2022 Oct;37(10):2106-2113.e1. doi: 10.1016/j.arth.2022.05.006. Epub 2022 May 6. J Arthroplasty. 2022. PMID: 35533820 Free PMC article.
-
No difference between CT- and MRI-based patient-specific instrumentation for total knee arthroplasty: an updated systematic review and meta-analysis.Front Bioeng Biotechnol. 2025 Jul 23;13:1624600. doi: 10.3389/fbioe.2025.1624600. eCollection 2025. Front Bioeng Biotechnol. 2025. PMID: 40771726 Free PMC article.
-
Spacer-based gap balancing is useful in total knee arthroplasty: a 3-year follow-up of a retrospective study.J Orthop Surg Res. 2021 Oct 21;16(1):633. doi: 10.1186/s13018-021-02788-6. J Orthop Surg Res. 2021. PMID: 34674736 Free PMC article.
References
-
- Czurda T, Fennema P, Baumgartner M, Ritschl P. The association between component malalignment and post-operative pain following navigation-assisted total knee arthroplasty: results of a cohort/nested case-control study. Knee Surg Sports Traumatol Arthrosc. 2010;18(7):863–869. doi: 10.1007/s00167-009-0990-y. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
