

A portable magnetofluidic platform for detecting sexually transmitted infections and antimicrobial susceptibility
- PMID: 33980576
- PMCID: PMC8363034
- DOI: 10.1126/scitranslmed.abf6356
A portable magnetofluidic platform for detecting sexually transmitted infections and antimicrobial susceptibility
Abstract
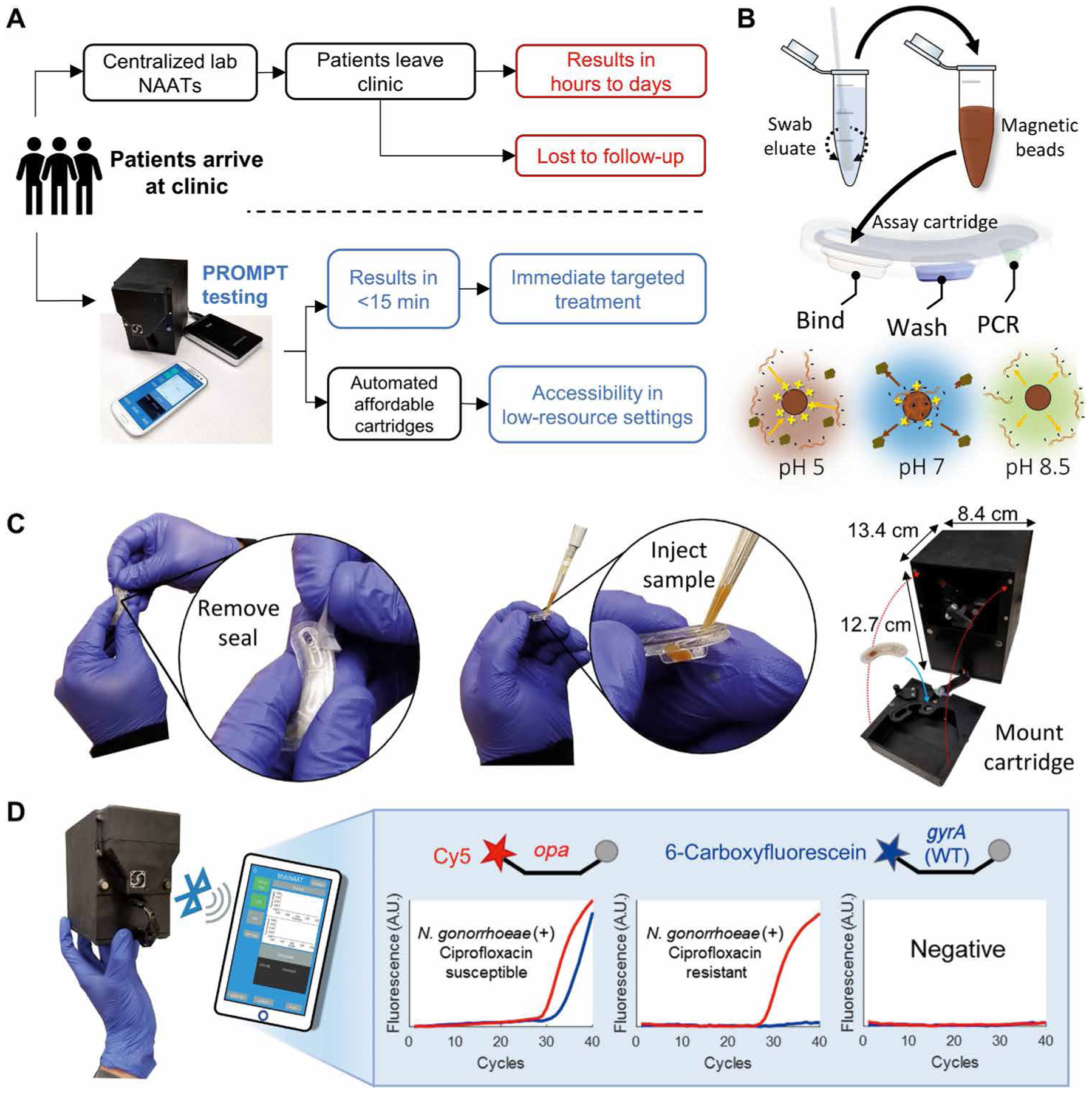
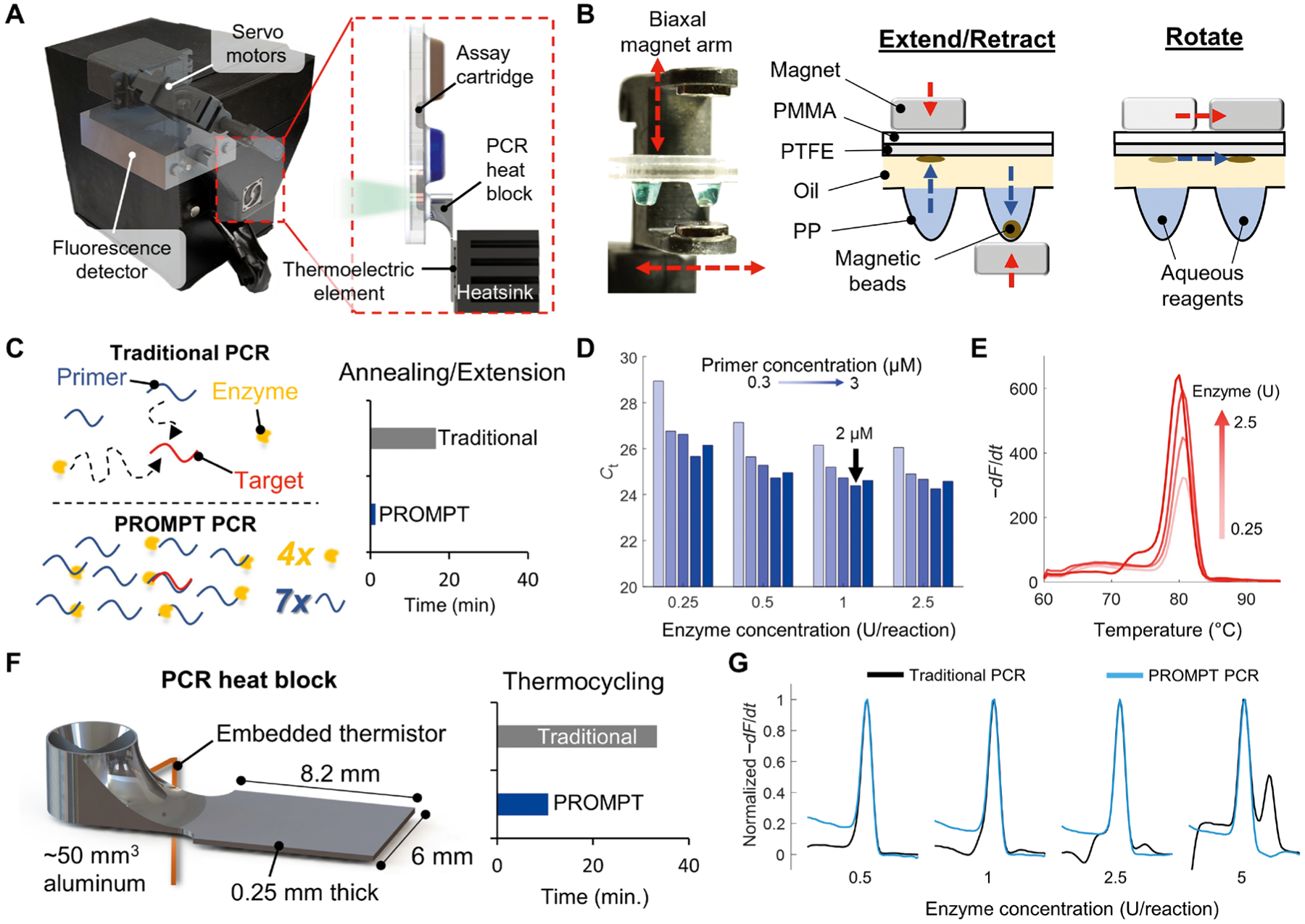
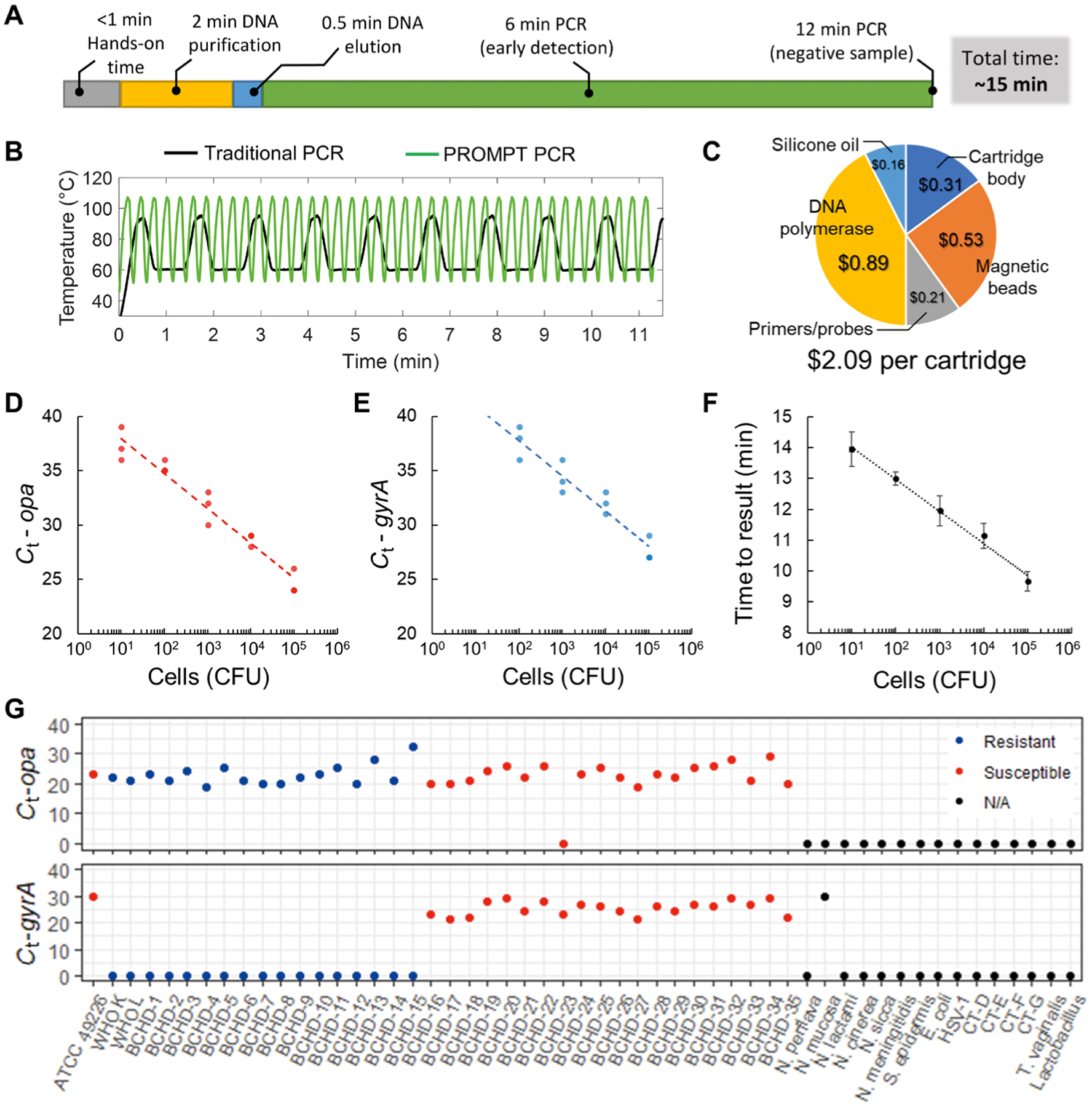
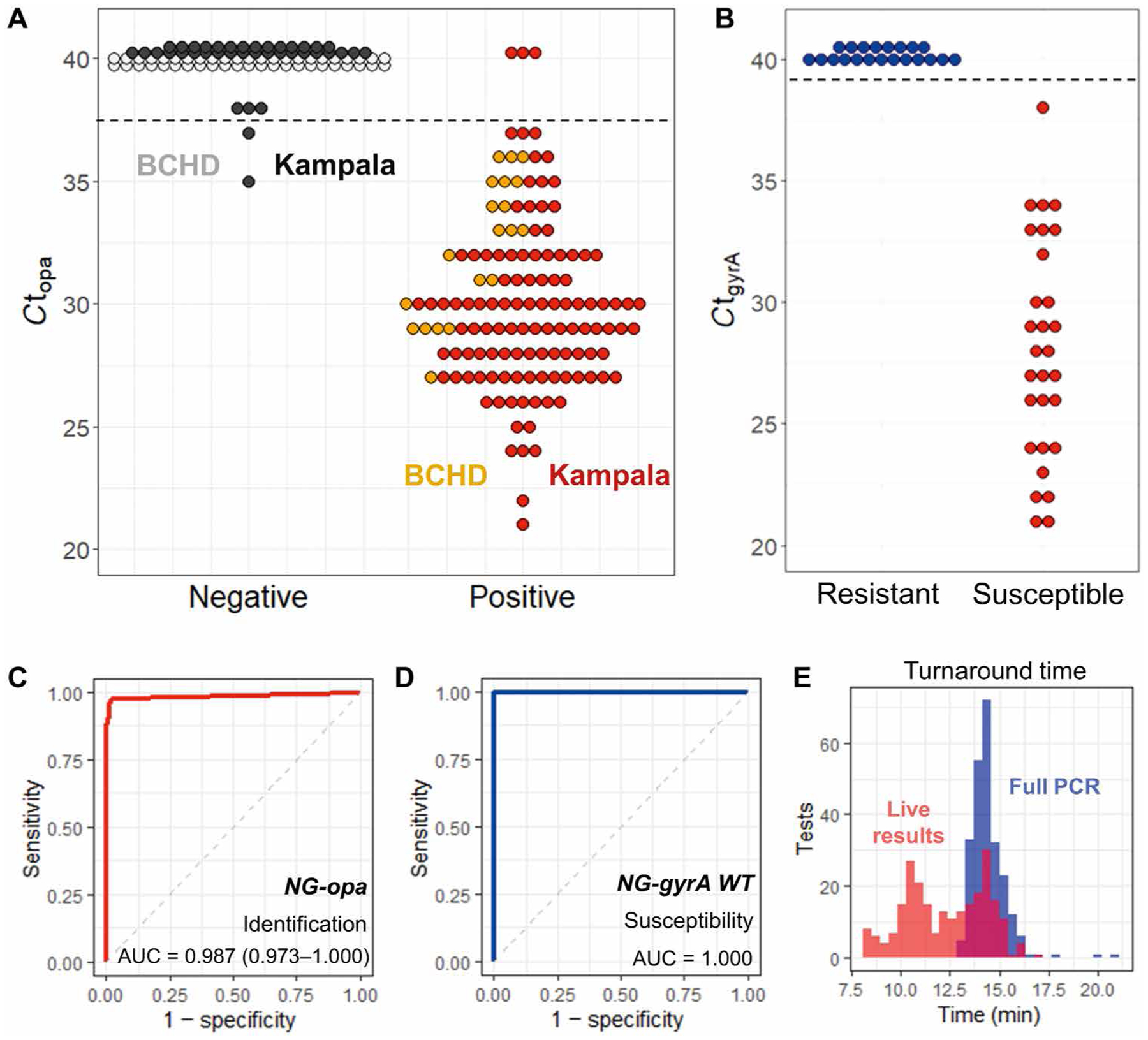
Effective treatment of sexually transmitted infections (STIs) is limited by diagnostics that cannot deliver results rapidly while the patient is still in the clinic. The gold standard methods for identification of STIs are nucleic acid amplification tests (NAATs), which are too expensive for widespread use and have lengthy turnaround times. To address the need for fast and affordable diagnostics, we have developed a portable, rapid, on-cartridge magnetofluidic purification and testing (PROMPT) polymerase chain reaction (PCR) test. We show that it can detect Neisseria gonorrhoeae, the pathogen causing gonorrhea, with simultaneous genotyping of the pathogen for resistance to the antimicrobial drug ciprofloxacin in <15 min. The duplex test was integrated into a low-cost thermoplastic cartridge with automated processing of penile swab samples from patients using magnetic beads. A compact instrument conducted DNA extraction, PCR, and analysis of results while relaying data to the user via a smartphone app. This platform was tested on penile swab samples from sexual health clinics in Baltimore, MD, USA (n = 66) and Kampala, Uganda (n = 151) with an overall sensitivity and specificity of 97.7% (95% CI, 94.7 to 100%) and 97.6% (95% CI, 94.1 to 100%), respectively, for N. gonorrhoeae detection and 100% concordance with culture results for ciprofloxacin resistance. This study paves the way for delivering accessible PCR diagnostics for rapidly detecting STIs at the point of care, helping to guide treatment decisions and combat the rise of antimicrobial resistant pathogens.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Competing interests:
A.Y.T. and T.-H.W. are co-inventors on patent PCT/US2019/029937 “A disposable reagent scaffold for biochemical process integration” that is associated with this study.
Figures
Comment in
-
A PROMPT response to STIs.Nat Rev Urol. 2021 Jul;18(7):384. doi: 10.1038/s41585-021-00492-y. Nat Rev Urol. 2021. PMID: 34127836 No abstract available.
Similar articles
-
Evaluation of self-collected samples in contrast to practitioner-collected samples for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by polymerase chain reaction among women living in remote areas.Sex Transm Dis. 2002 Nov;29(11):647-54. doi: 10.1097/00007435-200211000-00006. Sex Transm Dis. 2002. PMID: 12438900
-
The prevalence and antibiotics susceptibility pattern of Neisseria gonorrhoeae in patients attending OPD clinics at St. Mary's Hospital Lacor Uganda.J Prev Med Hyg. 2012 Dec;53(4):186-9. J Prev Med Hyg. 2012. PMID: 23469585
-
Conventional versus molecular detection of Chlamydia trachomatis and Neisseria gonorrhoeae among males in a sexually transmitted infections clinic.Malays J Pathol. 2017 Apr;39(1):25-31. Malays J Pathol. 2017. PMID: 28413202
-
Point-of-Care Testing for Sexually Transmitted Infections: A Review of Recent Developments.Arch Pathol Lab Med. 2020 Nov 1;144(11):1344-1351. doi: 10.5858/arpa.2020-0118-RA. Arch Pathol Lab Med. 2020. PMID: 32810868 Free PMC article. Review.
-
Expanding U.S. Laboratory Capacity for Neisseria gonorrhoeae Antimicrobial Susceptibility Testing and Whole-Genome Sequencing through the CDC's Antibiotic Resistance Laboratory Network.J Clin Microbiol. 2020 Mar 25;58(4):e01461-19. doi: 10.1128/JCM.01461-19. Print 2020 Mar 25. J Clin Microbiol. 2020. PMID: 32024723 Free PMC article. Review.
Cited by
-
Bridging the gap between development of point-of-care nucleic acid testing and patient care for sexually transmitted infections.Lab Chip. 2022 Feb 1;22(3):476-511. doi: 10.1039/d1lc00665g. Lab Chip. 2022. PMID: 35048928 Free PMC article. Review.
-
Automated and miniaturized screening of antibiotic combinations via robotic-printed combinatorial droplet platform.Acta Pharm Sin B. 2024 Apr;14(4):1801-1813. doi: 10.1016/j.apsb.2023.11.027. Epub 2023 Nov 28. Acta Pharm Sin B. 2024. PMID: 38572105 Free PMC article.
-
Increasing Access To Sexually Transmitted Infection Testing: The Promise of Point-of-Care and Over-the-Counter Tests.Curr HIV/AIDS Rep. 2025 Mar 25;22(1):27. doi: 10.1007/s11904-025-00736-1. Curr HIV/AIDS Rep. 2025. PMID: 40128446 Free PMC article. Review.
-
Smart toilets for monitoring COVID-19 surges: passive diagnostics and public health.NPJ Digit Med. 2022 Mar 30;5(1):39. doi: 10.1038/s41746-022-00582-0. NPJ Digit Med. 2022. PMID: 35354937 Free PMC article.
-
Advances in point-of-care genetic testing for personalized medicine applications.Biomicrofluidics. 2023 May 3;17(3):031501. doi: 10.1063/5.0143311. eCollection 2023 May. Biomicrofluidics. 2023. PMID: 37159750 Free PMC article. Review.
References
-
- Hull S, Kelley S, Clarke JL, Sexually transmitted infections: Compelling case for an improved screening strategy. Popul. Health Manag 20, S-1–S-11 (2017). - PubMed
-
- Rowley J, Vander Hoorn S, Korenromp E, Low N, Unemo M, Abu-Raddad LJ, Chico RM, Smolak A, Newman L, Gottlieb S, Thwin SS, Broutet N, Taylor MM, Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ 97, 548–562 (2019). - PMC - PubMed
-
- Unemo M, Golparian D, Eyre DW, Antimicrobial resistance in Neisseria gonorrhoeae and treatment of gonorrhea, in Neisseria gonorrhoeae, Methods in Molecular Biology, Christodoulides M, Ed. (Humana, 2019), vol. 1997, pp. 37–58. - PubMed
-
- Alirol E, Wi TE, Bala M, Bazzo ML, Chen XS, Deal C, Dillon JAR, Kularatne R, Heim J, Hooft van Huijsduijnen R, Hook EW, Lahra MM, Lewis DA, Ndowa F, Shafer WM, Tayler L, Workowski K, Unemo M, Balasegaram M, Multidrug-resistant gonorrhea: A research and development roadmap to discover new medicines. PLOS Med. 14, e1002366 (2017). - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
