

Simulating the computational mechanisms of cognitive and behavioral psychotherapeutic interventions: insights from active inference
- PMID: 33980875
- PMCID: PMC8115057
- DOI: 10.1038/s41598-021-89047-0
Simulating the computational mechanisms of cognitive and behavioral psychotherapeutic interventions: insights from active inference
Abstract
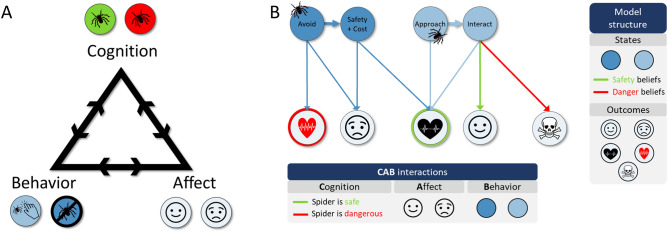
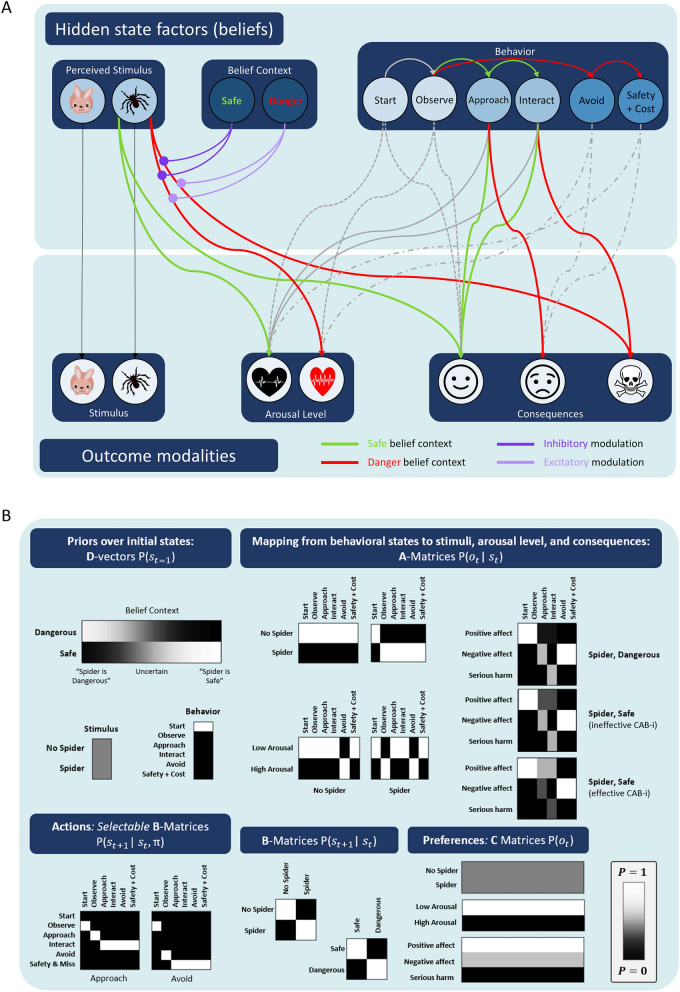
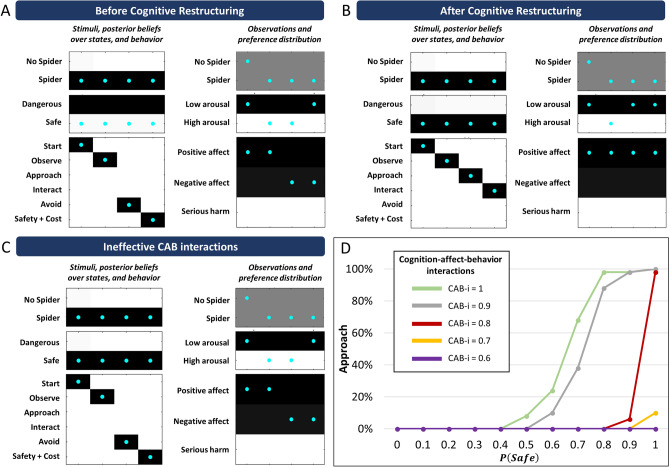
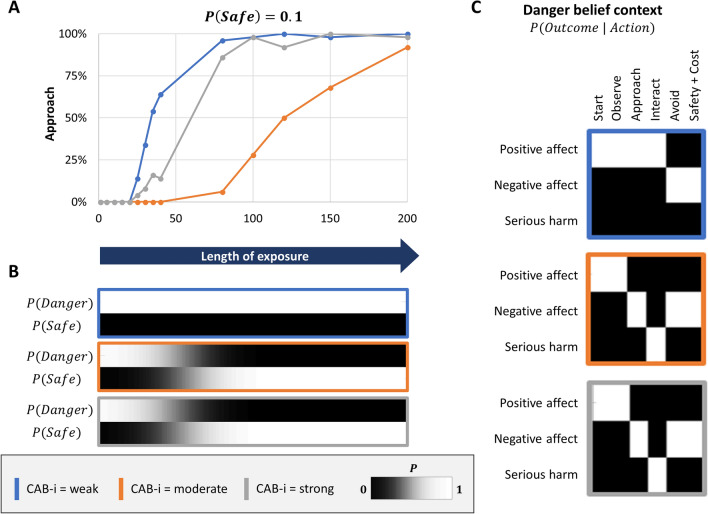
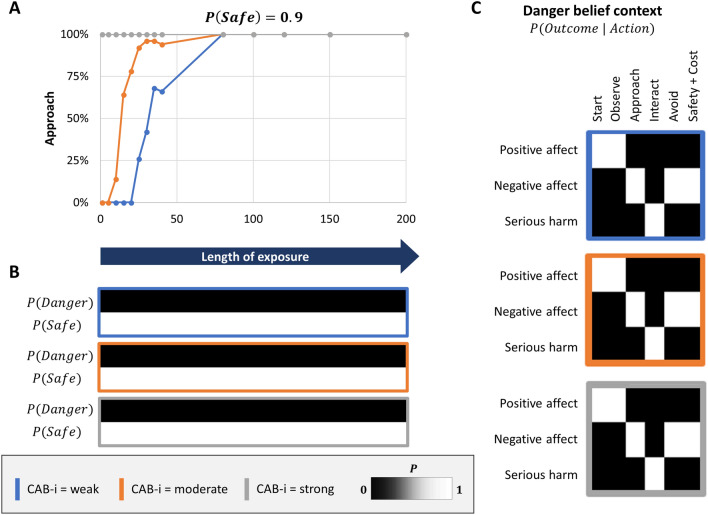
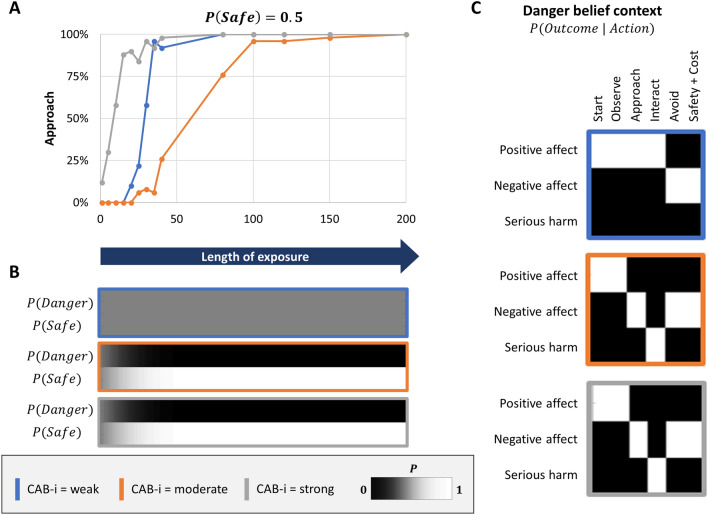
Cognitive-behavioral therapy (CBT) leverages interactions between thoughts, feelings, and behaviors. To deepen understanding of these interactions, we present a computational (active inference) model of CBT that allows formal simulations of interactions between cognitive interventions (i.e., cognitive restructuring) and behavioral interventions (i.e., exposure) in producing adaptive behavior change (i.e., reducing maladaptive avoidance behavior). Using spider phobia as a concrete example of maladaptive avoidance more generally, we show simulations indicating that when conscious beliefs about safety/danger have strong interactions with affective/behavioral outcomes, behavioral change during exposure therapy is mediated by changes in these beliefs, preventing generalization. In contrast, when these interactions are weakened, and cognitive restructuring only induces belief uncertainty (as opposed to strong safety beliefs), behavior change leads to generalized learning (i.e., "over-writing" the implicit beliefs about action-outcome mappings that directly produce avoidance). The individual is therefore equipped to face any new context, safe or dangerous, remaining in a content state without the need for avoidance behavior-increasing resilience from a CBT perspective. These results show how the same changes in behavior during CBT can be due to distinct underlying mechanisms; they predict lower rates of relapse when cognitive interventions focus on inducing uncertainty and on reducing the effects of automatic negative thoughts on behavior.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Acceptance and mindfulness-based cognitive-behavioral therapies].Sante Ment Que. 2013 Autumn;38(2):35-63. doi: 10.7202/1023989ar. Sante Ment Que. 2013. PMID: 24719002 French.
-
"Change the mind and you change the brain": effects of cognitive-behavioral therapy on the neural correlates of spider phobia.Neuroimage. 2003 Feb;18(2):401-9. doi: 10.1016/s1053-8119(02)00030-7. Neuroimage. 2003. PMID: 12595193
-
Change in Seasonal Beliefs Mediates the Durability Advantage of Cognitive-Behavioral Therapy Over Light Therapy for Winter Depression.Behav Ther. 2023 Jul;54(4):682-695. doi: 10.1016/j.beth.2022.11.002. Epub 2022 Dec 7. Behav Ther. 2023. PMID: 37330257 Clinical Trial.
-
Overall goal of Cognitive-Behavioral Therapy in Major Psychiatric Disorders and Suicidality: A Narrative Review.Med Clin North Am. 2023 Jan;107(1):143-167. doi: 10.1016/j.mcna.2022.05.006. Epub 2022 Oct 28. Med Clin North Am. 2023. PMID: 36402496 Review.
-
[Focused Cognitive Therapy: A New Possibility for the Treatment of Depression].Psychiatr Hung. 2019;34(4):369-379. Psychiatr Hung. 2019. PMID: 31767797 Review. Hungarian.
Cited by
-
The role of affective states in computational psychiatry.Int J Neuropsychopharmacol. 2025 Aug 1;28(8):pyaf049. doi: 10.1093/ijnp/pyaf049. Int J Neuropsychopharmacol. 2025. PMID: 40600644 Free PMC article. Review.
-
Tracking and changing beliefs during social interaction: Where computational psychiatry meets cognitive behavioral therapy.Front Psychol. 2022 Oct 7;13:1010012. doi: 10.3389/fpsyg.2022.1010012. eCollection 2022. Front Psychol. 2022. PMID: 36275316 Free PMC article. No abstract available.
-
The Association Between Doctor-Patient Conflict and Uncertainty Stress During Clinical Internships Among Medical Students: A Panel Study.Healthcare (Basel). 2025 May 6;13(9):1080. doi: 10.3390/healthcare13091080. Healthcare (Basel). 2025. PMID: 40361858 Free PMC article.
-
Active Inference in Psychology and Psychiatry: Progress to Date?Entropy (Basel). 2024 Sep 30;26(10):833. doi: 10.3390/e26100833. Entropy (Basel). 2024. PMID: 39451909 Free PMC article. Review.
-
Lower Levels of Directed Exploration and Reflective Thinking Are Associated With Greater Anxiety and Depression.Front Psychiatry. 2022 Jan 7;12:782136. doi: 10.3389/fpsyt.2021.782136. eCollection 2021. Front Psychiatry. 2022. PMID: 35126200 Free PMC article.
References
-
- Beck, J. Cognitive behavior therapy: Basics and beyond. (2011).
-
- APA. Presidential task force on evidence-based practice. Evidence-based practice in psychology. American Psychologist61, 271–285, doi:10.1037/0003-066X.61.4.271 (2006). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
