

Clinical course and risk factors of fatal adverse outcomes in COVID-19 patients in Korea: a nationwide retrospective cohort study
- PMID: 33980912
- PMCID: PMC8115137
- DOI: 10.1038/s41598-021-89548-y
Clinical course and risk factors of fatal adverse outcomes in COVID-19 patients in Korea: a nationwide retrospective cohort study
Abstract
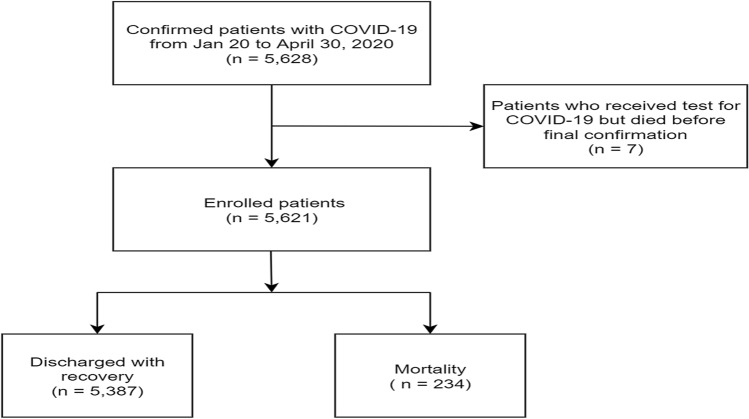
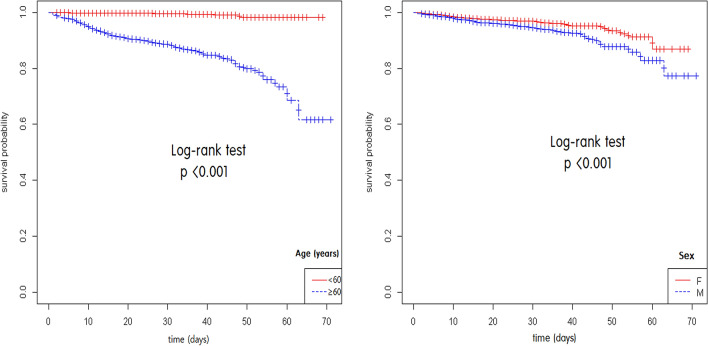
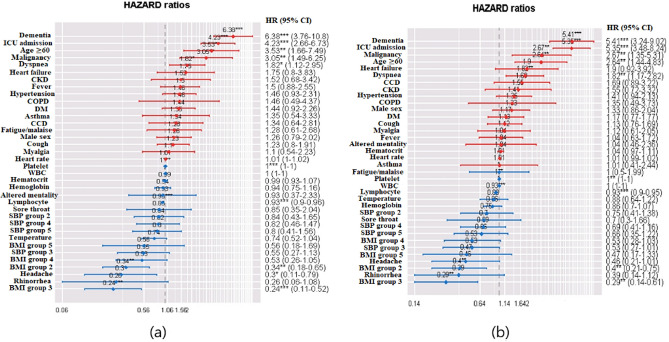
We investigated association between epidemiological and clinical characteristics of coronavirus disease 2019 (COVID-19) patients and clinical outcomes in Korea. This nationwide retrospective cohort study included 5621 discharged patients with COVID-19, extracted from the Korea Disease Control and Prevention Agency (KDCA) database. We compared clinical data between survivors (n = 5387) and non-survivors (n = 234). We used logistic regression analysis and Cox proportional hazards model to explore risk factors of death and fatal adverse outcomes. Increased odds ratio (OR) of mortality occurred with age (≥ 60 years) [OR 11.685, 95% confidence interval (CI) 4.655-34.150, p < 0.001], isolation period, dyspnoea, altered mentality, diabetes, malignancy, dementia, and intensive care unit (ICU) admission. The multivariable regression equation including all potential variables predicted mortality (AUC = 0.979, 95% CI 0.964-0.993). Cox proportional hazards model showed increasing hazard ratio (HR) of mortality with dementia (HR 6.376, 95% CI 3.736-10.802, p < 0.001), ICU admission (HR 4.233, 95% CI 2.661-6.734, p < 0.001), age ≥ 60 years (HR 3.530, 95% CI 1.664-7.485, p = 0.001), malignancy (HR 3.054, 95% CI 1.494-6.245, p = 0.002), and dyspnoea (HR 1.823, 95% CI 1.125-2.954, p = 0.015). Presence of dementia, ICU admission, age ≥ 60 years, malignancy, and dyspnoea could help clinicians identify COVID-19 patients with poor prognosis.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical Characteristics and Outcomes of COVID-19 Cohort Patients in Daegu Metropolitan City Outbreak in 2020.J Korean Med Sci. 2021 Jan 4;36(1):e12. doi: 10.3346/jkms.2021.36.e12. J Korean Med Sci. 2021. PMID: 33398946 Free PMC article.
-
Risk factors for adverse clinical outcomes with COVID-19 in China: a multicenter, retrospective, observational study.Theranostics. 2020 May 15;10(14):6372-6383. doi: 10.7150/thno.46833. eCollection 2020. Theranostics. 2020. PMID: 32483458 Free PMC article.
-
Characteristics in Pediatric Patients with Coronavirus Disease 2019 in Korea.J Korean Med Sci. 2021 May 24;36(20):e148. doi: 10.3346/jkms.2021.36.e148. J Korean Med Sci. 2021. PMID: 34032033 Free PMC article.
-
Clinical Outcomes of COVID-19 Patients with Type 2 Diabetes: A Population-Based Study in Korea.Endocrinol Metab (Seoul). 2020 Dec;35(4):901-908. doi: 10.3803/EnM.2020.787. Epub 2020 Dec 10. Endocrinol Metab (Seoul). 2020. PMID: 33297603 Free PMC article.
-
Outcomes among patients with COVID-19 and asthma: A systematic review and meta-analysis.Allergy Asthma Proc. 2021 Jul 1;42(4):267-273. doi: 10.2500/aap.2021.42.210041. Allergy Asthma Proc. 2021. PMID: 34187619
Cited by
-
Risk factors for poor prognosis in children and adolescents with COVID-19: A systematic review and meta-analysis.EClinicalMedicine. 2021 Nov;41:101155. doi: 10.1016/j.eclinm.2021.101155. Epub 2021 Oct 19. EClinicalMedicine. 2021. PMID: 34693233 Free PMC article.
-
Risk factors for hospitalization and death due to COVID-19 among frail community-dwelling elderly people: a retrospective cohort study.Sao Paulo Med J. 2022 Sep-Oct;140(5):676-681. doi: 10.1590/1516-3180.2021.0649.R1.20122021. Sao Paulo Med J. 2022. PMID: 35976369 Free PMC article.
-
Efficacy and Safety of Complementary Therapy With Jing Si Herbal Tea in Patients With Mild-To-Moderate COVID-19: A Prospective Cohort Study.Front Nutr. 2022 Mar 14;9:832321. doi: 10.3389/fnut.2022.832321. eCollection 2022. Front Nutr. 2022. PMID: 35369061 Free PMC article.
-
Single nucleotide variants in the CCL2, OAS1 and DPP9 genes and their association with the severity of COVID-19 in an Ecuadorian population.Front Cell Infect Microbiol. 2024 Apr 17;14:1322882. doi: 10.3389/fcimb.2024.1322882. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38694517 Free PMC article.
-
Retrospective Evaluation of the Efficacy of Combined Antiviral Therapy Versus Monotherapy in High-Risk Hospitalized COVID-19 Patients.Cureus. 2025 Apr 8;17(4):e81903. doi: 10.7759/cureus.81903. eCollection 2025 Apr. Cureus. 2025. PMID: 40342453 Free PMC article.
References
-
- Coronavirus Resource Center. Coronavirus COVID‐19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University, https://coronavirus.jhu.edu/map.html (2020).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
