

COVID-19's natural course among ambulatory monitored outpatients
- PMID: 33980931
- PMCID: PMC8115337
- DOI: 10.1038/s41598-021-89545-1
COVID-19's natural course among ambulatory monitored outpatients
Abstract
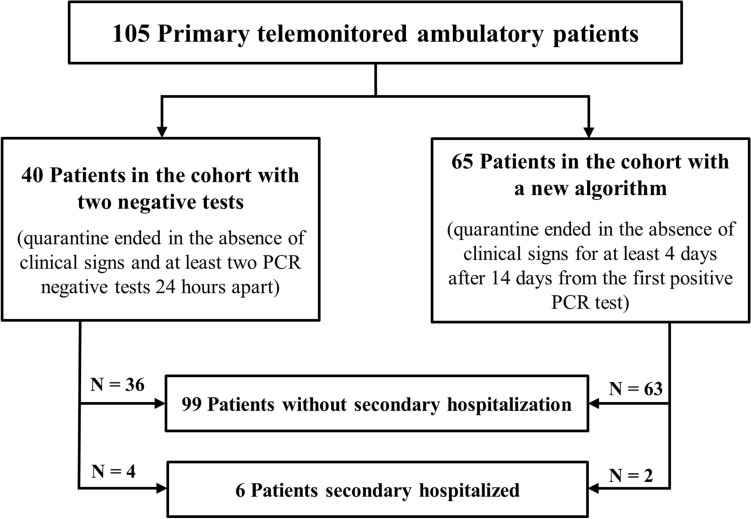
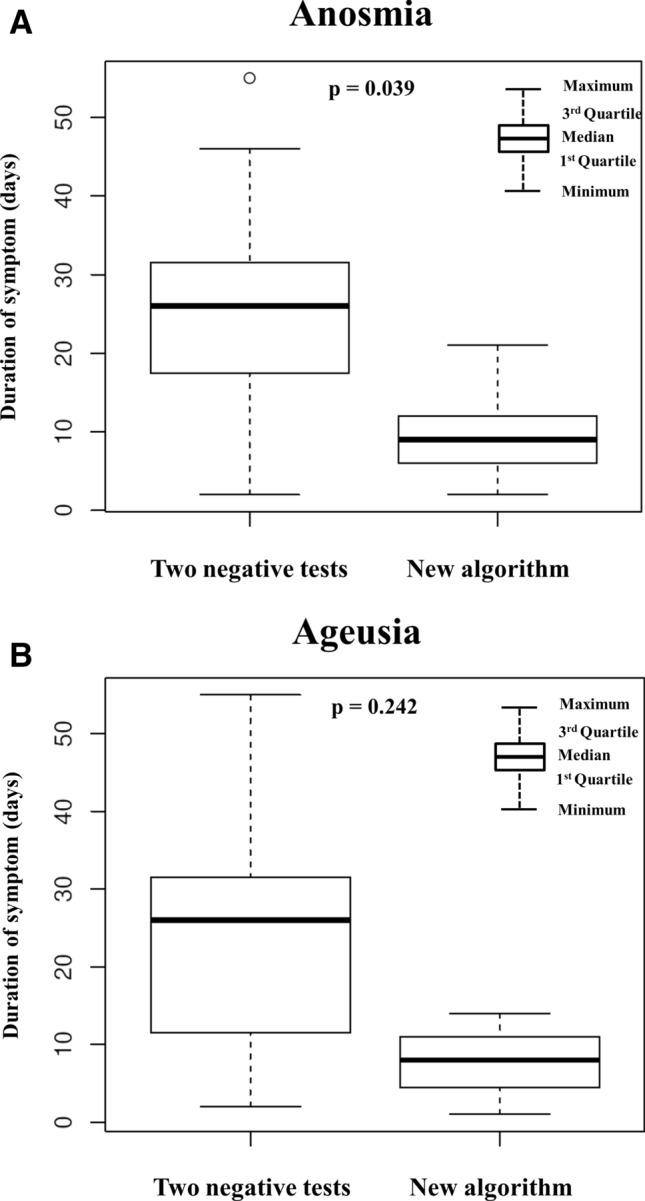
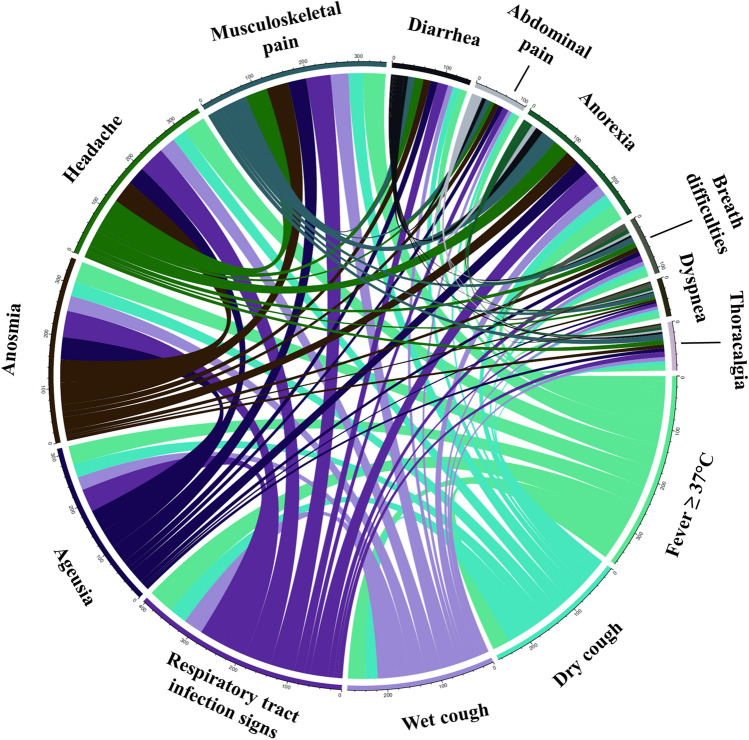
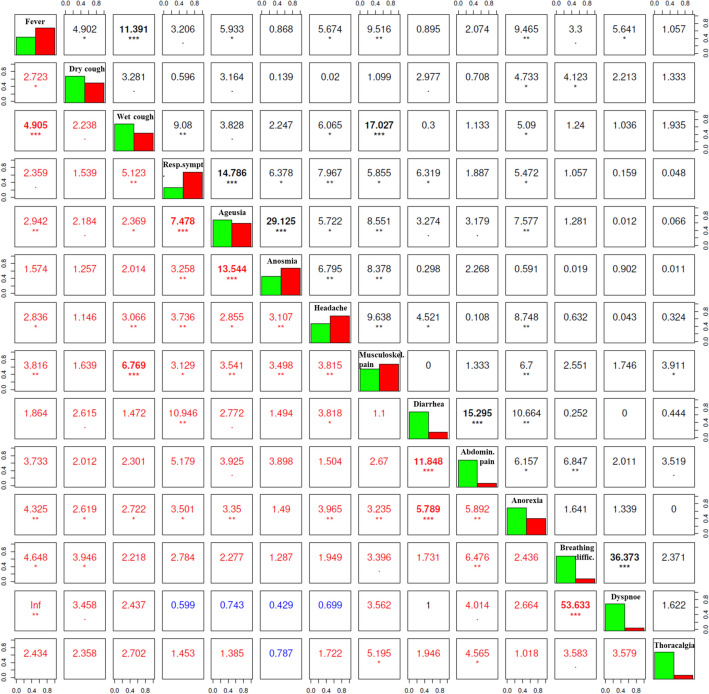
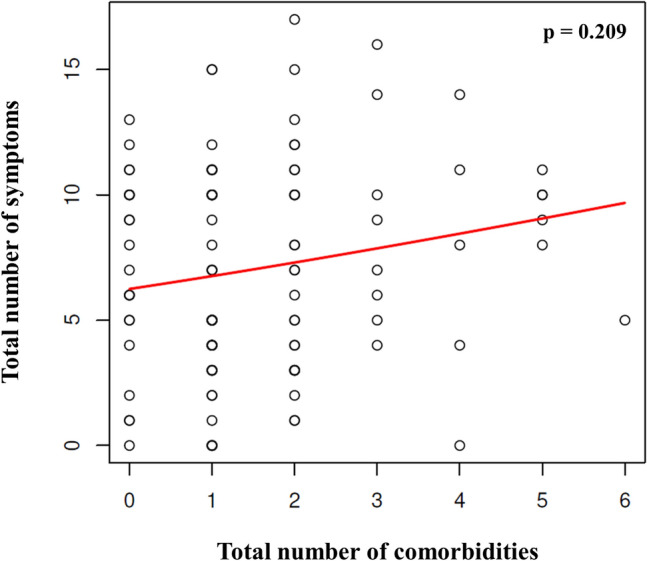
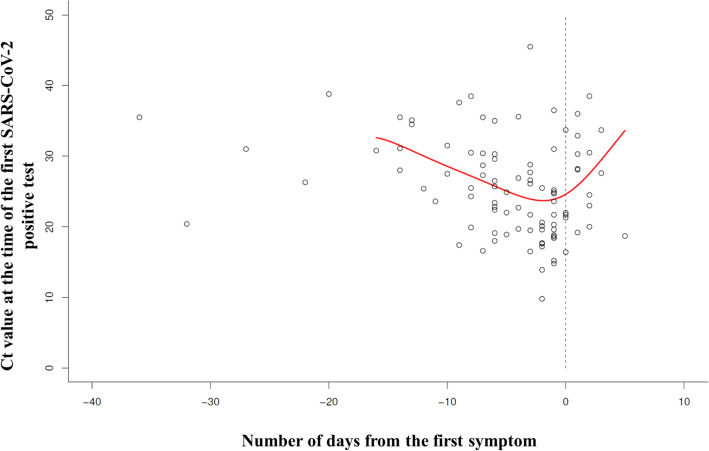
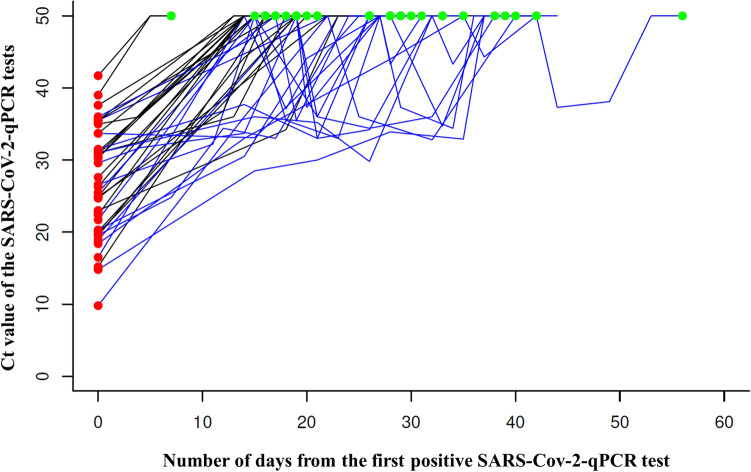
Research objective was to detail COVID-19's natural trajectory in relation to the Czech population's viral load. Our prospective detailed daily questionnaire-based telemonitoring study evaluated COVID-19's impact among 105 outpatients. In accordance with government quarantine requirements, outpatients were divided into a cohort with two negative tests at the end of the disease (40 patients) and a cohort with a new algorithm (65 patients) following a 14-day quarantine. Median follow-up differed significantly between the 2 groups (23 days vs. 16 days). Only 6% of patients were asymptomatic during the entire telemonitoring period. Another 13% of patients were diagnosed asymptomatic, as suspected contacts, yet later developed symptoms, while the remaining 81% were diagnosed as symptomatic on average 6 days following symptom onset. Telemonitoring enabled precise symptom status chronicling. The most frequently reported complaints were fevers, respiratory issues, and anosmia. Six patients were eventually hospitalized for complications detected early after routine telemonitoring. During the extended follow-up (median 181 days), anosmia persisted in 26% of patients. 79% of patients in the new quarantine algorithm cohort reported no symptoms on day 11 compared to just 56% of patients in the two negative test cohort upon first testing negative (median-19 days). The highest viral load occurred within 0-2 days of initial symptom onset. Both the PCR viral load and two consecutive PCR negative sample realizations indicated high interindividual variability with a surprisingly fluctuating pattern among 43% of patients. No definitive COVID-19 symptoms or set of symptoms excepting anosmia (59%) and/or ageusia (47%) were identified. No preexisting medical conditions specifically foreshadowed disease trajectory in a given patient. Without a PCR negativity requirement for quarantine cessation, patients could exhibit fewer symptoms. Our study therefore highlights the urgent need for routine ambulatory patient telemedicine monitoring, early complication detection, intensive mass education connecting disease demeanor with subsequent swift diagnostics, and, notably, the need to reevaluate and modify quarantine regulations for better control of SARS-CoV-2 proliferation.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO. Coronavirus disease (COVID-19) pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 20 Dec 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
