

An artificial intelligence system for predicting the deterioration of COVID-19 patients in the emergency department
- PMID: 33980980
- PMCID: PMC8115328
- DOI: 10.1038/s41746-021-00453-0
An artificial intelligence system for predicting the deterioration of COVID-19 patients in the emergency department
Abstract
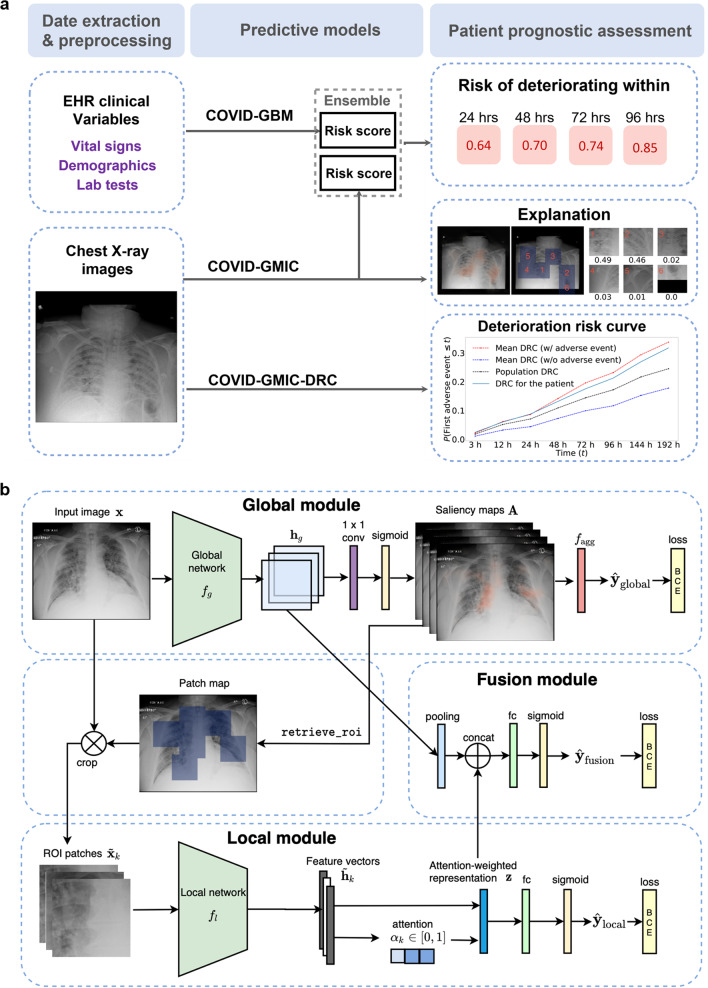
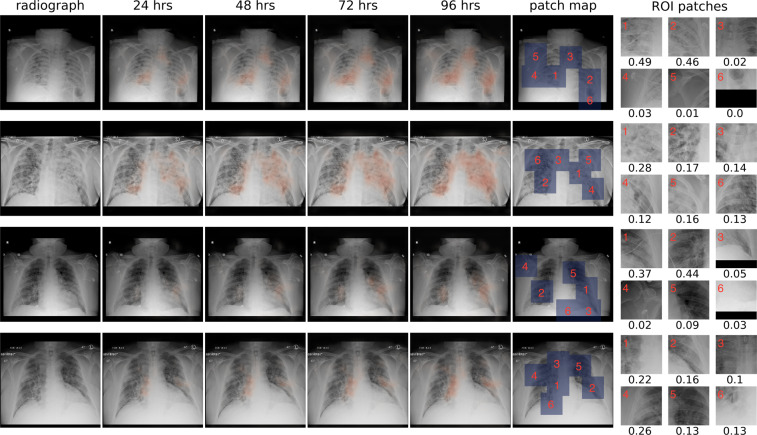
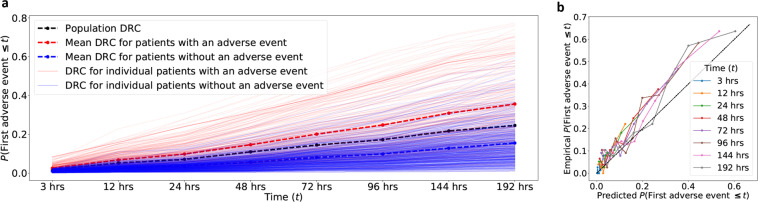
During the coronavirus disease 2019 (COVID-19) pandemic, rapid and accurate triage of patients at the emergency department is critical to inform decision-making. We propose a data-driven approach for automatic prediction of deterioration risk using a deep neural network that learns from chest X-ray images and a gradient boosting model that learns from routine clinical variables. Our AI prognosis system, trained using data from 3661 patients, achieves an area under the receiver operating characteristic curve (AUC) of 0.786 (95% CI: 0.745-0.830) when predicting deterioration within 96 hours. The deep neural network extracts informative areas of chest X-ray images to assist clinicians in interpreting the predictions and performs comparably to two radiologists in a reader study. In order to verify performance in a real clinical setting, we silently deployed a preliminary version of the deep neural network at New York University Langone Health during the first wave of the pandemic, which produced accurate predictions in real-time. In summary, our findings demonstrate the potential of the proposed system for assisting front-line physicians in the triage of COVID-19 patients.
Conflict of interest statement
The authors declare no competing interests.
Figures

Update of
-
An artificial intelligence system for predicting the deterioration of COVID-19 patients in the emergency department.ArXiv [Preprint]. 2020 Nov 4:arXiv:2008.01774v2. ArXiv. 2020. Update in: NPJ Digit Med. 2021 May 12;4(1):80. doi: 10.1038/s41746-021-00453-0. PMID: 32793769 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
