

A comparative evaluation of Advanced Platelet-Rich Fibrin (A-PRF) and Platelet-Rich Fibrin (PRF) as a Scaffold in Regenerative Endodontic Treatment of Traumatized Immature Non-vital permanent anterior teeth: A Prospective clinical study
- PMID: 33981393
- PMCID: PMC8106940
- DOI: 10.4317/jced.57902
A comparative evaluation of Advanced Platelet-Rich Fibrin (A-PRF) and Platelet-Rich Fibrin (PRF) as a Scaffold in Regenerative Endodontic Treatment of Traumatized Immature Non-vital permanent anterior teeth: A Prospective clinical study
Abstract
Background: Regenerative endodontic treatment (RET) is a promising treatment alternative for traumatized immature non-vital teeth. Advanced platelet-rich fibrin (A-PRF) contains significantly more growth factors than Platelet-rich fibrin (PRF) and has not been evaluated as a scaffold in RET. The aim of the present study was to evaluate and compare A-PRF and PRF as scaffolds in the RET concerning periapical healing, and root development of traumatized immature non-vital teeth.
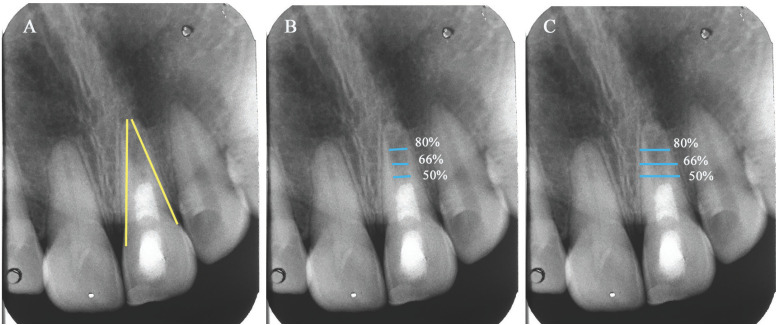
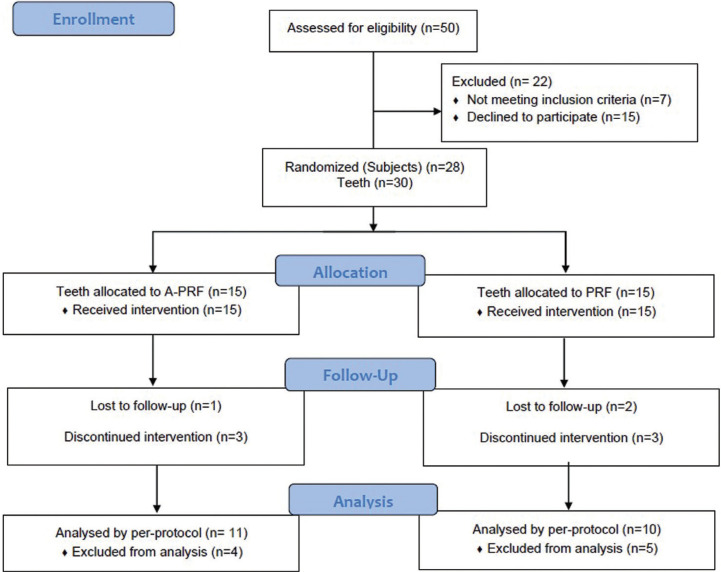
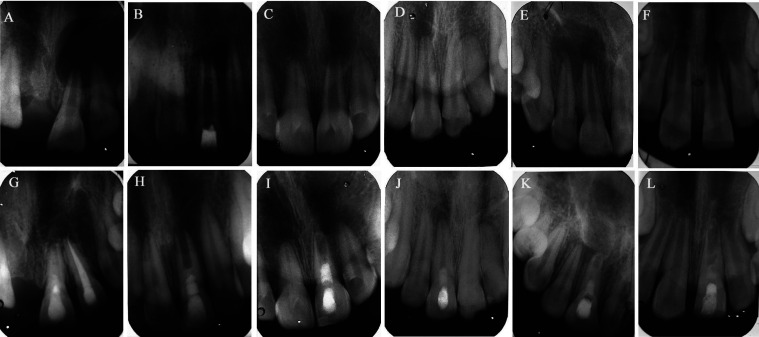
Material and methods: In the present study, RET was performed on 30 traumatized immature non-vital maxillary incisors in 28 patients aged between 8-27 years. Minimal mechanical debridement and irrigation with 1.5% sodium hypochlorite and 17% ethylenediaminetetraacetic acid was performed. Canals were disinfected using modified triple antibiotic paste consisting of ciprofloxacin, metronidazole and cefaclor. Based on the type of scaffold, teeth were randomly assigned into A-PRF (n=15) and PRF groups (n=15). Periapical healing, apical response and quantitative root dimensions (length and thickness) were analyzed radiographically after 12 months follow-up.
Results: Nineteen patients with 21 teeth (A-PRF n=11, PRF n=10) completed the follow-up and 9 patients were excluded. Clinically, patients in both the groups were asymptomatic. The survival rates for A-PRF and PRF were 78.5% and 77.5%, respectively. No statistically significant differences were detected between A-PRF and PRF regarding periapical healing and type of apical response (p& 0.05). The difference in the pre-operative and follow-up root thickness and root length in both A-PRF and PRF groups were statistically significant (p< 0.05).
Conclusions: Based on short-term results of 13 months, both A-PRF and PRF can be used as scaffold in regenerative endodontic treatment of traumatized immature non-vital teeth. A-PRF could be recommended in such cases since it yielded more root dentin thickness which is crucial for reinforcing immature teeth. Key words:Regenerative endodontic treatment, dental trauma, Non-vital teeth, immature teeth, platelet-rich fibrin, advanced platelet-rich fibrin.
Copyright: © 2021 Medicina Oral S.L.
Conflict of interest statement
Conflicts of interest Veena Jayadevan declares that she has no conflict of interest. Paras Mull Gehlot declares that he has no conflict of interest. Vinutha Manjunath declares that she has no conflict of interest. Subbarao V Madhunapantula declares that he has no conflict of interest. Jyothi Swandenahalli Lakshmikanth declares that she has no conflict of interest.
Figures

References
-
- Trope M. Treatment of the immature tooth with a non-vital pulp and apical periodontitis. Dent Clin North Am. 2010;54:313–324. - PubMed
-
- Lin J, Zeng Q, Wei X, Zhao W, Cui M, Gu J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J Endod. 2017;43:1821–7. - PubMed
-
- Diogenes A, Ruparel N. Regenerative Endodontic Procedures: Clinical Outcomes. Dent Clin N Am. 2017;61:111–125. - PubMed
-
- Chen M, Chen K, Chen C, Tayebaty F, Rosenberg P, Lin L. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int Endod J. 2012;45:294–305. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous