

Finite element analysis of subtalar joint arthroereisis on adult-acquired flexible flatfoot deformity using customised sinus tarsi implant
- PMID: 33981572
- PMCID: PMC8071640
- DOI: 10.1016/j.jot.2020.02.004
Finite element analysis of subtalar joint arthroereisis on adult-acquired flexible flatfoot deformity using customised sinus tarsi implant
Abstract
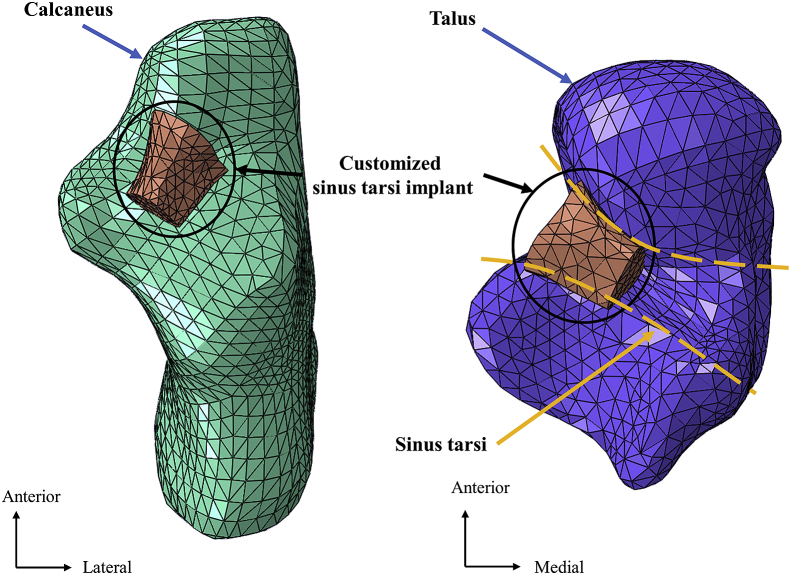
Background: Subtalar arthroereisis may cause sinus tarsi pain complications. In this study, we aimed to introduce a customised implant that facilitated treatment effect and less impingement. The biomechanical outcome between the intact and implant conditions was compared using finite element analysis.
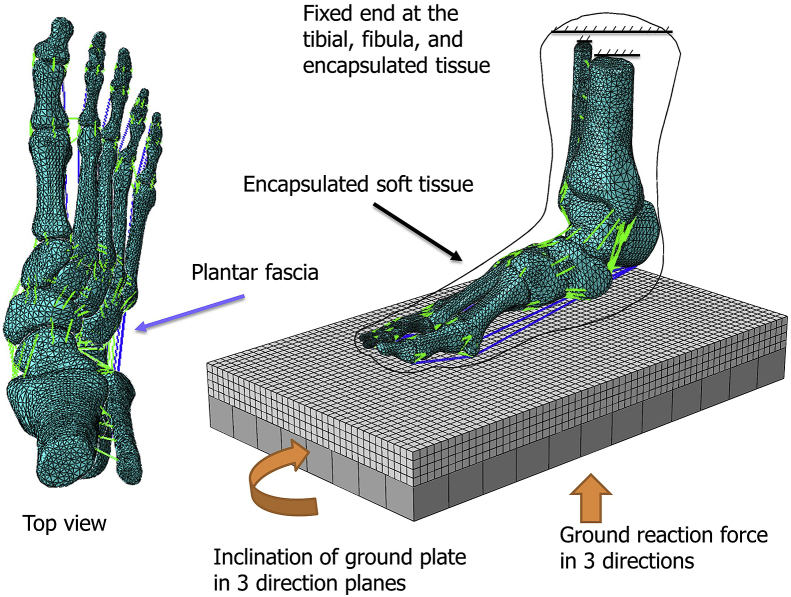
Methods: A female patient with flatfoot (age: 36 years, height: 156 cm, body mass: 51 kg) was recruited as the model patient. The customised implant was designed from the extracted geometry. Boundary and loading conditions were assumed from the data of a normal participant. Four gait instants, including the ground reaction force first peak (25% stance), valley (45%), initial push-off (60%) and second peak (75%) were analyzed.
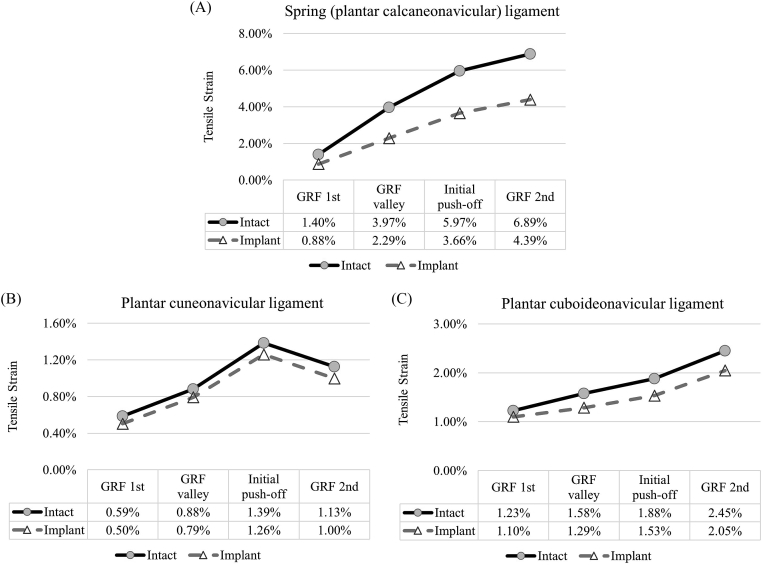
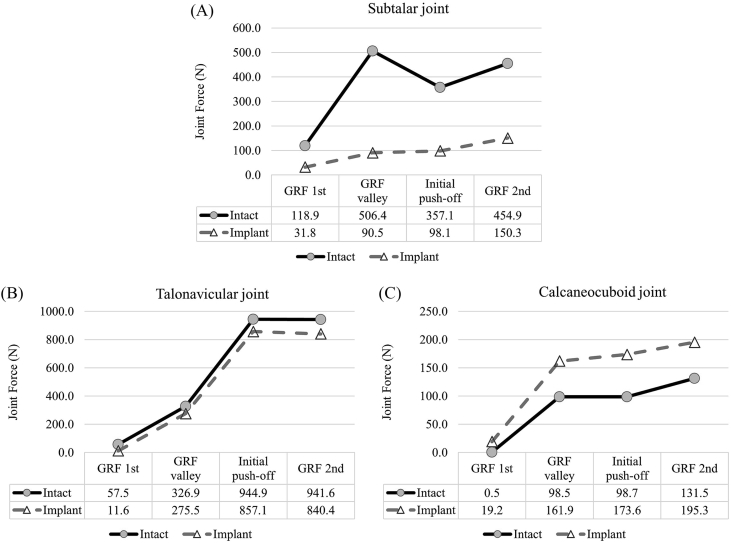
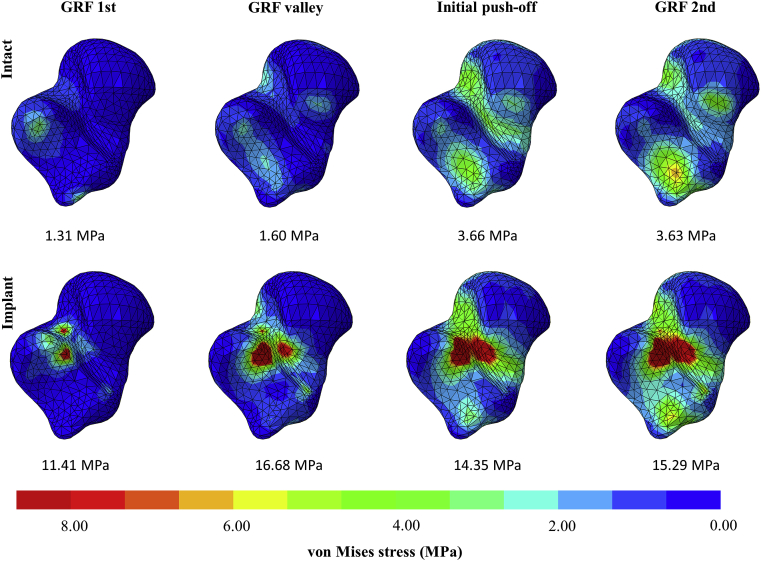
Results: The navicular height was elevated by 4.2% at 25% stance, whereas the strain of the spring, plantar cuneonavicular and plantar cuboideonavicular ligaments were reduced. The talonavicular joint force decreased and the calcaneocuboid joint increased by half and 67%, respectively, representing a lateralised load pathway. There was a stress concentration at the sulcus tali reaching 15.29 MPa.
Conclusion: Subtalar arthroereisis using a customised implant may produce some positive treatment effects in terms of navicular height elevation, ligament strain relief and lateralised joint loading pathway. Although the concentrated stress at the sulcus tali did not exceed the threshold of bone breakdown, we could not rule out the potential of vascular disturbance owing to the remarkable elevation of stress. Future study may enlarge the contact area of the bone-implant interface by considering customisation based on the dynamic change of the sinus tarsi during walking gait.
The translational potential of this article: Geometry mismatch of prefabricated implants could be the reason for complications. With the advancement of 3D printing, customising implant becomes possible and may improve treatment outcome. This study implemented a theoretical model approach to explore its potential under a simulation of walking.
Keywords: Extra-osseous talotarsal stabilisation; Pes planus; Posterior tibial tendon dysfunction; Sinus tarsi implant; Talotarsal mechanism.
© 2020 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose in relation to this article.
Figures
Similar articles
-
Response to the letter to editor regarding "finite element analysis of subtalar joint arthroereisis on adult acquired flexible flatfoot deformity using customized sinus tarsi implant".J Orthop Translat. 2022 Dec 9;37:173-174. doi: 10.1016/j.jot.2022.12.002. eCollection 2022 Nov. J Orthop Translat. 2022. PMID: 36569456 Free PMC article. No abstract available.
-
Biomechanical consequences of subtalar joint arthroereisis in treating posterior tibial tendon dysfunction: a theoretical analysis using finite element analysis.Comput Methods Biomech Biomed Engin. 2017 Nov;20(14):1525-1532. doi: 10.1080/10255842.2017.1382484. Epub 2017 Sep 27. Comput Methods Biomech Biomed Engin. 2017. PMID: 28952799
-
Comparison of Extraosseous Talotarsal Stabilization Implants in a Stage II Adult-Acquired Flatfoot Model: A Finite Element Analysis.J Foot Ankle Surg. 2017 Sep-Oct;56(5):1058-1064. doi: 10.1053/j.jfas.2017.05.009. Epub 2017 Jun 13. J Foot Ankle Surg. 2017. PMID: 28623061
-
Arthroereisis: Treatment of Pes Planus.Cureus. 2022 Jan 7;14(1):e21003. doi: 10.7759/cureus.21003. eCollection 2022 Jan. Cureus. 2022. PMID: 35154977 Free PMC article. Review.
-
Operative treatment of the difficult stage 2 adult acquired flatfoot deformity.Foot Ankle Clin. 2001 Mar;6(1):95-119. doi: 10.1016/s1083-7515(03)00083-4. Foot Ankle Clin. 2001. PMID: 11385931 Review.
Cited by
-
Letter to the editor regarding "Finite element analysis of subtalar joint arthroereisis on adult-acquired flexible flatfoot deformity using customised sinus tarsi implant".J Orthop Translat. 2022 Mar 3;33:70-71. doi: 10.1016/j.jot.2022.02.003. eCollection 2022 Mar. J Orthop Translat. 2022. PMID: 35281521 Free PMC article. No abstract available.
-
Anatomical Features of the Tarsal Sinus in Patients with Pes Planus: Implications for Clinical Management.Med Sci Monit. 2023 Sep 21;29:e940687. doi: 10.12659/MSM.940687. Med Sci Monit. 2023. PMID: 37731240 Free PMC article.
-
Finite element stress analysis of the hindfoot after medial displacement calcaneal osteotomy with different translation distances.Med Biol Eng Comput. 2025 Jul;63(7):1955-1964. doi: 10.1007/s11517-025-03309-x. Epub 2025 Feb 3. Med Biol Eng Comput. 2025. PMID: 39894893
-
Response to the letter to editor regarding "finite element analysis of subtalar joint arthroereisis on adult acquired flexible flatfoot deformity using customized sinus tarsi implant".J Orthop Translat. 2022 Dec 9;37:173-174. doi: 10.1016/j.jot.2022.12.002. eCollection 2022 Nov. J Orthop Translat. 2022. PMID: 36569456 Free PMC article. No abstract available.
-
Comparison of different surgical treatments for stage II progressive collapsing foot deformity: a finite element analysis.J Orthop Surg Res. 2023 Sep 23;18(1):719. doi: 10.1186/s13018-023-04216-3. J Orthop Surg Res. 2023. PMID: 37741994 Free PMC article.
References
-
- Graham M.E., Jawrani N.T., Chikka A. Extraosseous talotarsal stabilization using HyProCure® in adults: a 5-year retrospective follow-up. J Foot Ankle Surg. 2012;51(1):23–29. - PubMed
-
- Graham M.E., Jawrani N.T., Chikka A., Rogers R.J. Surgical treatment of hyperpronation using an extraosseous talotarsal stabilization device: radiographic outcomes in 70 adult patients. J Foot Ankle Surg. 2012;51(5):548–555. - PubMed
-
- Graham M.E., Jawrani N.T., Goel V.K. Effect of extra-osseous talotarsal stabilization on posterior tibial nerve strain in hyperpronating feet: a cadaveric evaluation. J Foot Ankle Surg. 2011;50(6):672–675. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
