

The role of imaging in acute pancreatitis
- PMID: 33982269
- PMCID: PMC8292294
- DOI: 10.1007/s11547-021-01359-3
The role of imaging in acute pancreatitis
Abstract
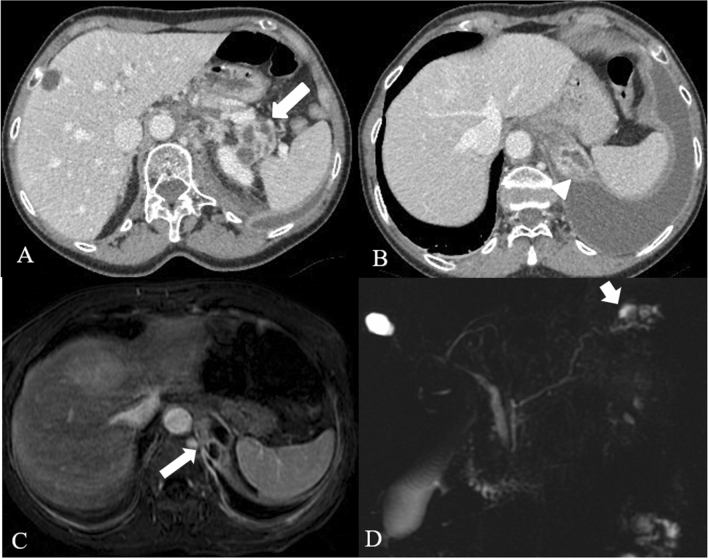
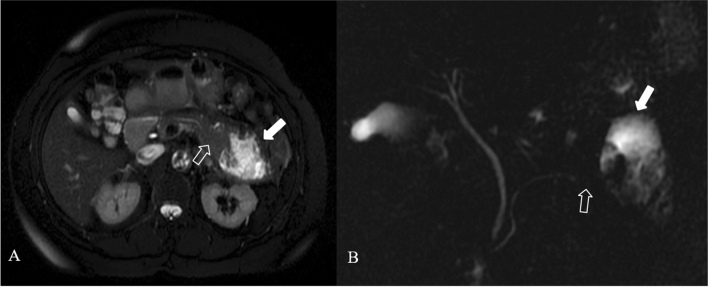
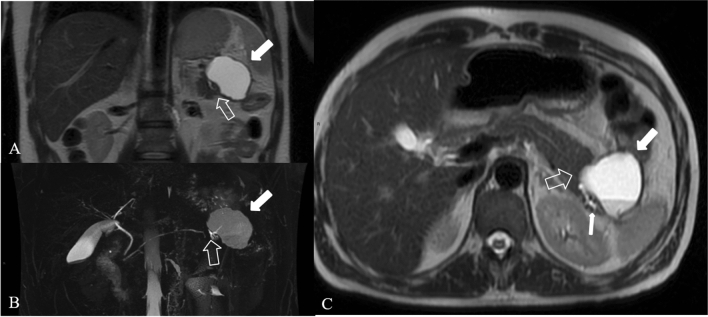
Acute pancreatitis is one of the most commonly encountered etiologies in the emergency setting, with a broad spectrum of findings that varies in severity from mild interstitial pancreas to severe forms with significant local and systemic complications that are associated with a substantial degree of morbidity and mortality. In this article the radiological aspect of the terminology and classification of acute pancreatitis are reviewed. The roles of ultrasound, computed tomography, and magnetic resonance imaging in the diagnosis and evaluation of acute pancreatitis and its complications are discussed. The authors present a practical image-rich guide, applying the revised Atlanta classification system, with the goal of facilitating radiologists to write a correct report, and reinforcing the radiologist's role as a key member of a multidisciplinary team in treating patients with acute pancreatitis. Computed tomography is the most performed imaging test for acute pancreatitis. Nevertheless, MRI is useful in many specific situations, due to its superiority soft tissue contrast resolution and better assessment of biliary and pancreatic duct, for example in the ductal disconnection. The purpose if this article is to review recent advances in imaging acquisition and analytic techniques in the evaluation of AP.
Keywords: Acute pancreatitis; Computed tomography (CT); Interstitial edematous pancreatitis; MRI; Magnetic resonance cholangiopancreatography (MRCP); Necrotizing Pancreatitis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures











References
-
- Xiao AY, Tan ML, Wu LM, Asrani VM, Windsor JA, Yadav D, Petrov MS. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi: 10.1016/S2468-1253(16)30004-8. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
