

Assessing the Causal Relationships Between Insulin Resistance and Hyperuricemia and Gout Using Bidirectional Mendelian Randomization
- PMID: 33982892
- PMCID: PMC8568618
- DOI: 10.1002/art.41779
Assessing the Causal Relationships Between Insulin Resistance and Hyperuricemia and Gout Using Bidirectional Mendelian Randomization
Abstract
Objective: Hyperuricemia is closely associated with insulin resistance syndrome (and its many cardiometabolic sequelae); however, whether they are causally related has long been debated. We undertook this study to investigate the potential causal nature and direction between insulin resistance and hyperuricemia, along with gout, by using bidirectional Mendelian randomization (MR) analyses.
Methods: We used genome-wide association data (n = 288,649 for serum urate [SU] concentration; n = 763,813 for gout risk; n = 153,525 for fasting insulin) to select genetic instruments for 2-sample MR analyses, using multiple MR methods to address potential pleiotropic associations. We then used individual-level, electronic medical record-linked data from the UK Biobank (n = 360,453 persons of European ancestry) to replicate our analyses via single-sample MR analysis.
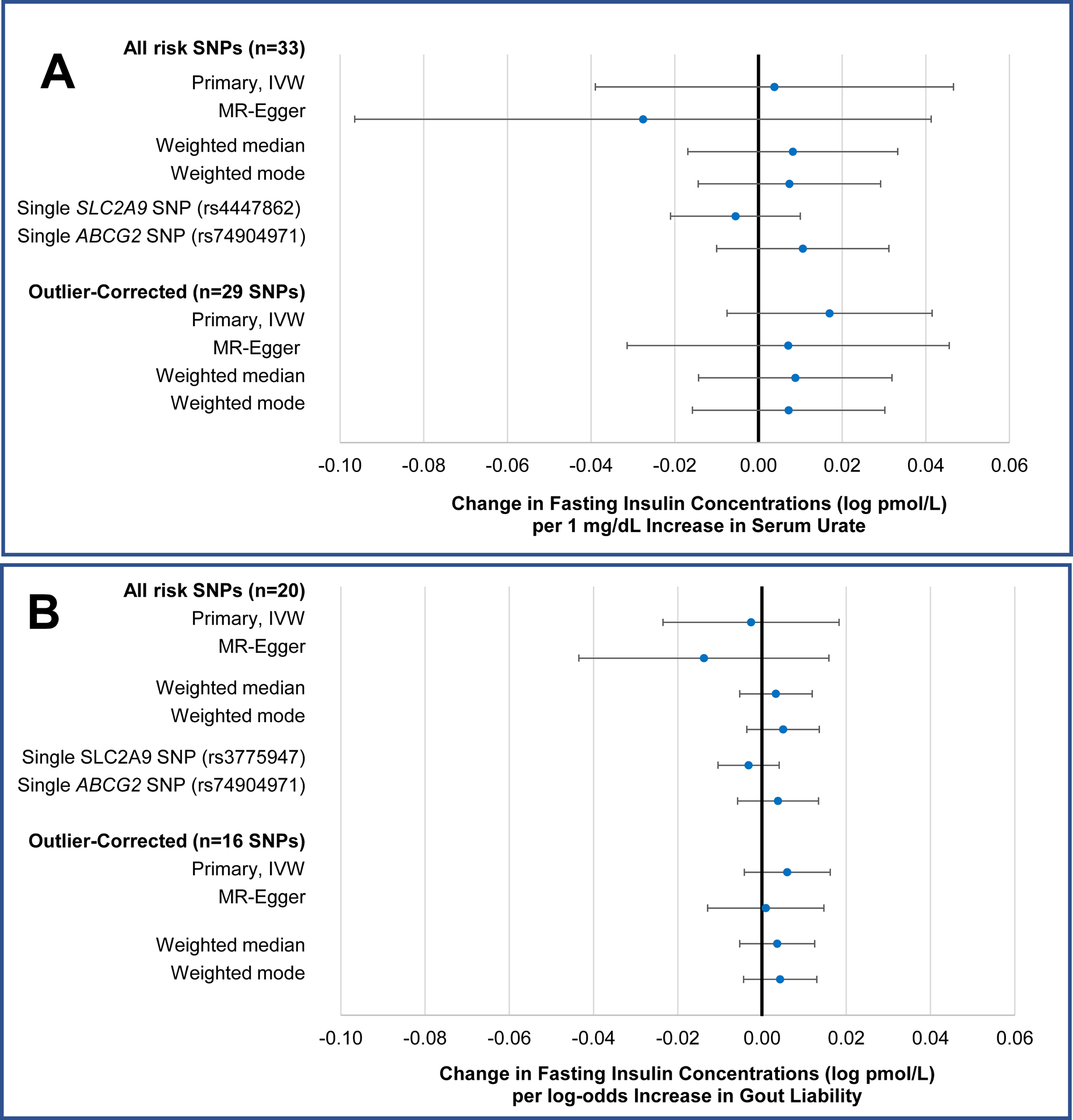
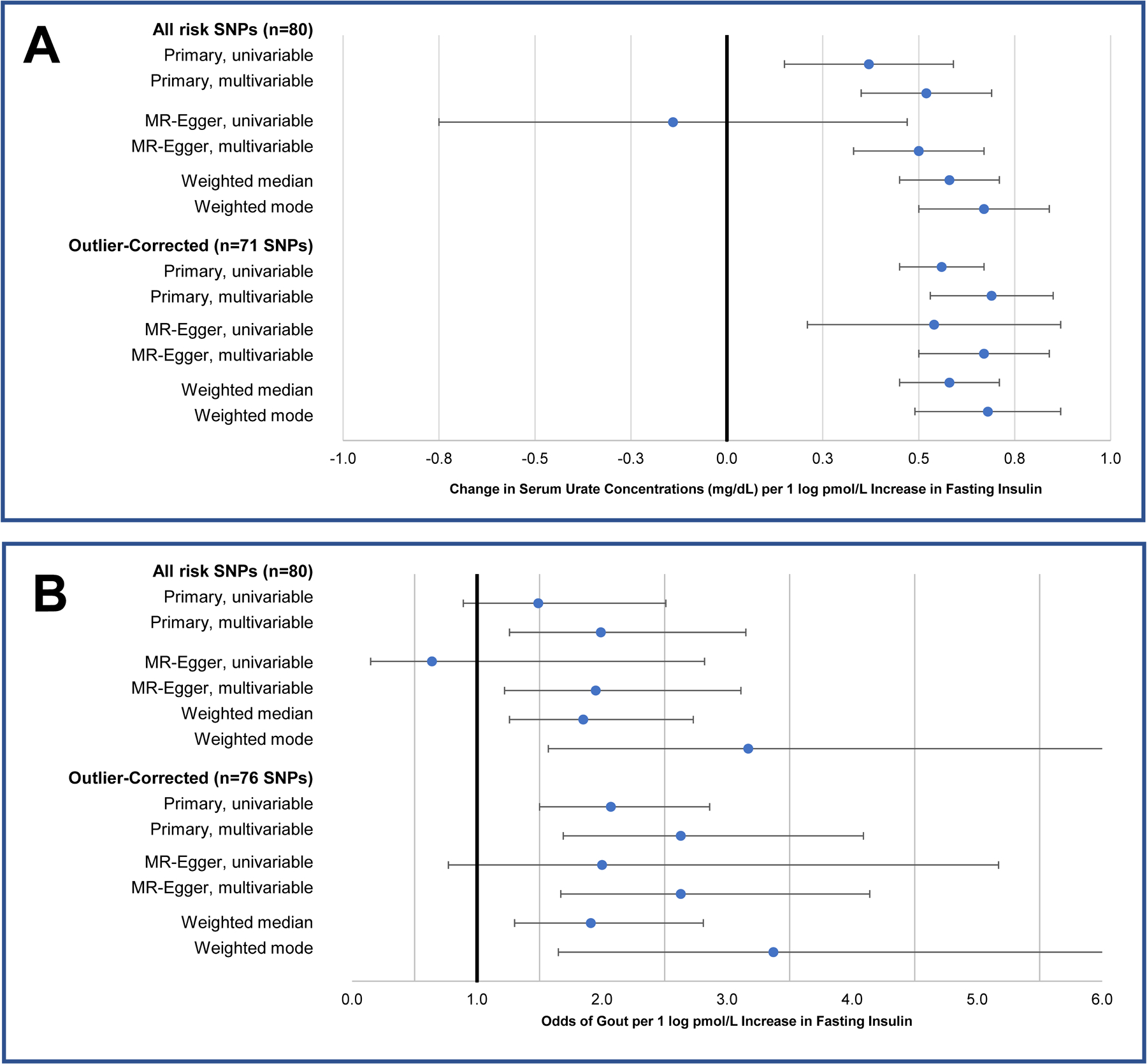
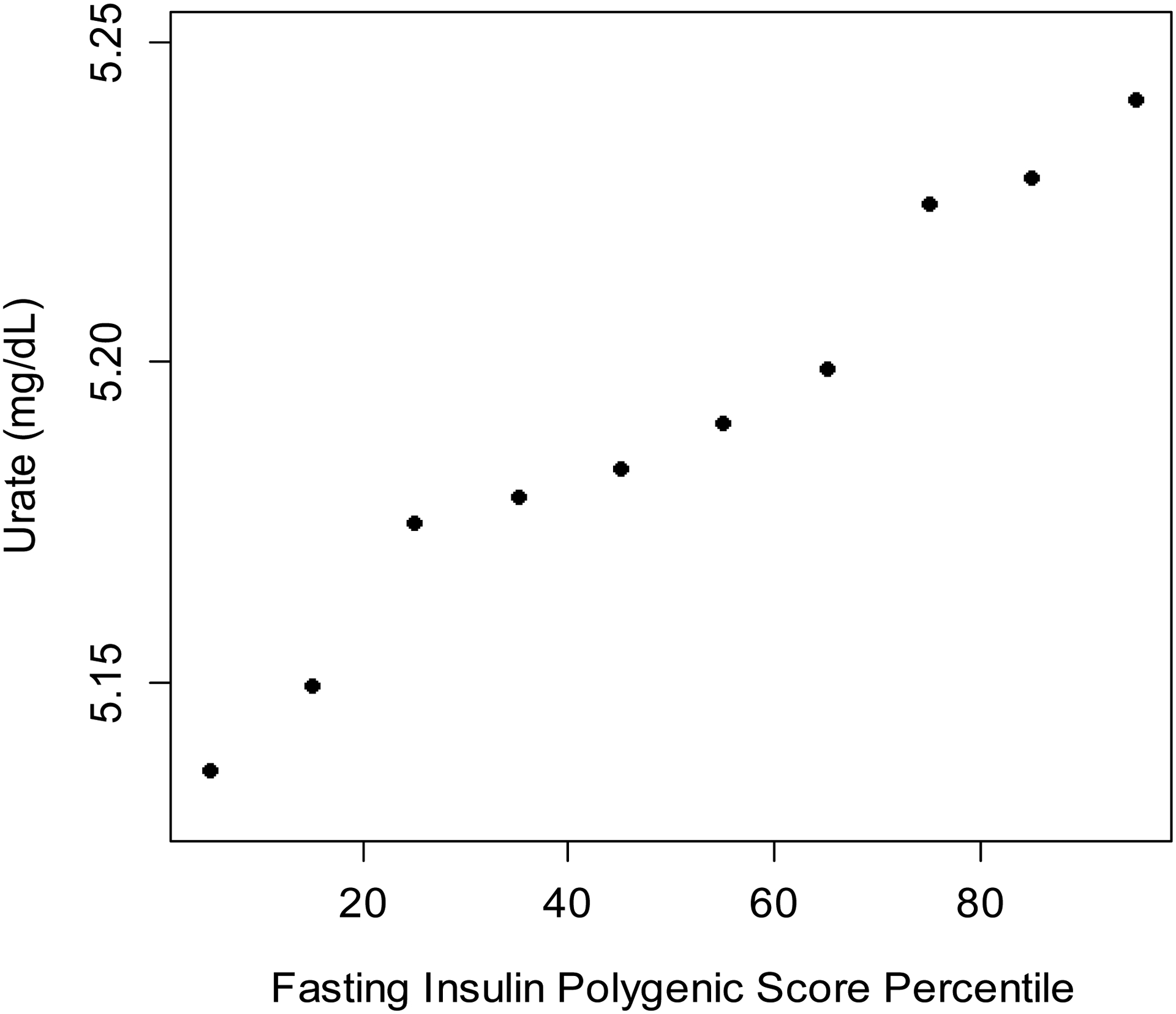
Results: Genetically determined SU levels, whether inferred from a polygenic score or strong individual loci, were not associated with fasting insulin concentrations. In contrast, genetically determined fasting insulin concentrations were positively associated with SU levels (0.37 mg/dl per log-unit increase in fasting insulin [95% confidence interval (95% CI) 0.15, 0.58]; P = 0.001). This persisted in outlier-corrected (β = 0.56 mg/dl [95% CI 0.45, 0.67]) and multivariable MR analyses adjusted for BMI (β = 0.69 mg/dl [95% CI 0.53, 0.85]) (P < 0.001 for both). Polygenic scores for fasting insulin were also positively associated with SU level among individuals in the UK Biobank (P < 0.001). Findings for gout risk were bidirectionally consistent with those for SU level.
Conclusion: These findings provide evidence to clarify core questions about the close association between hyperuricemia and insulin resistance syndrome: hyperinsulinemia leads to hyperuricemia but not the other way around. Reducing insulin resistance could lower the SU level and gout risk, whereas lowering the SU level (e.g., allopurinol treatment) is unlikely to mitigate insulin resistance and its cardiometabolic sequelae.
© 2021, American College of Rheumatology.
Figures
References
-
- Safiri S, Kolahi A-A, Cross M, Carson-Chahhoud K, Hoy D, Almasi-Hashiani A, et al. Prevalence, Incidence, and Years Lived With Disability Due to Gout and Its Attributable Risk Factors for 195 Countries and Territories 1990–2017: A Systematic Analysis of the Global Burden of Disease Study 2017. Arthritis Rheumatol Hoboken NJ 2020;72:1916–1927. - PubMed
-
- Choi HK, Ford ES. Prevalence of the metabolic syndrome in individuals with hyperuricemia. Am J Med 2007;120:442–447. - PubMed
-
- Zhu Y, Pandya BJ, Choi HK. Comorbidities of Gout and Hyperuricemia in the US General Population: NHANES 2007–2008. Am J Med 2012;125:679–687.e1. - PubMed
-
- Facchini F, Chen YD, Hollenbeck CB, Reaven GM. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA 1991;266:3008–3011. - PubMed
-
- Rathmann W, Funkhouser E, Dyer AR, Roseman JM. Relations of hyperuricemia with the various components of the insulin resistance syndrome in young black and white adults: the CARDIA study. Coronary Artery Risk Development in Young Adults. Ann Epidemiol 1998;8:250–261. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50-AR-060772/AR/NIAMS NIH HHS/United States
- T32 AR007258/AR/NIAMS NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- T32 DK110919/DK/NIDDK NIH HHS/United States
- R01 AR056291/AR/NIAMS NIH HHS/United States
- 2020096/DDCF/Doris Duke Charitable Foundation/United States
- CIHR/Canada
- T32-DK-110909/DK/NIDDK NIH HHS/United States
- Rheumatology Research Foundation
- R01-AR0-65944/AR/NIAMS NIH HHS/United States
- R01-AR-056291/AR/NIAMS NIH HHS/United States
- R01 AR065944/AR/NIAMS NIH HHS/United States
- P50 AR060772/AR/NIAMS NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- T32-AR-007258/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
