

Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Quality of Life and Cancer Control Among Older and Frail Patients With Advanced Gastroesophageal Cancer: The GO2 Phase 3 Randomized Clinical Trial
- PMID: 33983395
- PMCID: PMC8120440
- DOI: 10.1001/jamaoncol.2021.0848
Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Quality of Life and Cancer Control Among Older and Frail Patients With Advanced Gastroesophageal Cancer: The GO2 Phase 3 Randomized Clinical Trial
Erratum in
-
Error in Author Name.JAMA Oncol. 2021 Aug 1;7(8):1249. doi: 10.1001/jamaoncol.2021.2796. JAMA Oncol. 2021. PMID: 34165523 Free PMC article. No abstract available.
Abstract
Importance: Older and/or frail patients are underrepresented in landmark cancer trials. Tailored research is needed to address this evidence gap.
Objective: The GO2 randomized clinical trial sought to optimize chemotherapy dosing in older and/or frail patients with advanced gastroesophageal cancer, and explored baseline geriatric assessment (GA) as a tool for treatment decision-making.
Design, setting, and participants: This multicenter, noninferiority, open-label randomized trial took place at oncology clinics in the United Kingdom with nurse-led geriatric health assessment. Patients were recruited for whom full-dose combination chemotherapy was considered unsuitable because of advanced age and/or frailty.
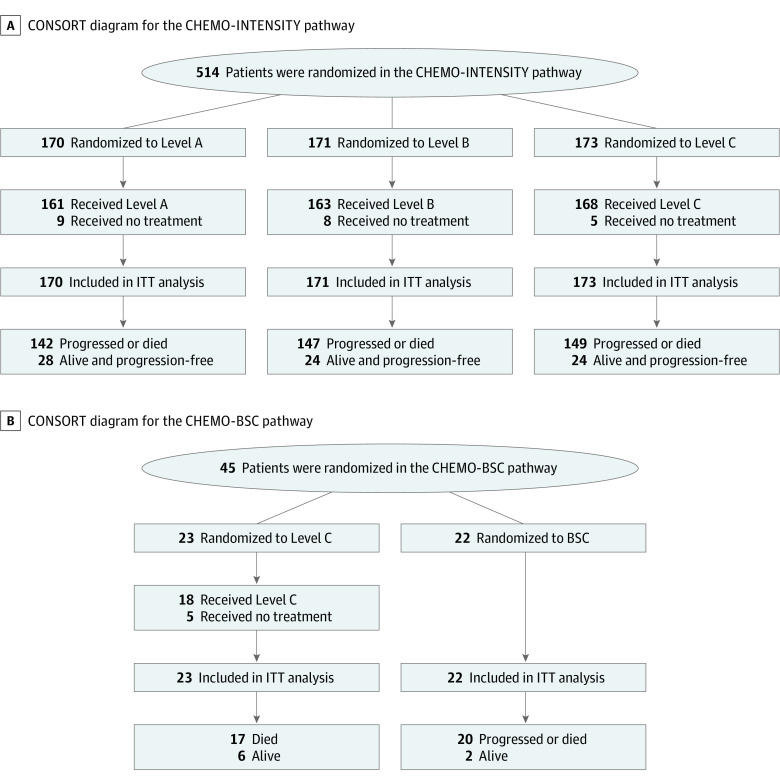
Interventions: There were 2 randomizations that were performed: CHEMO-INTENSITY compared oxaliplatin/capecitabine at Level A (oxaliplatin 130 mg/m2 on day 1, capecitabine 625 mg/m2 twice daily on days 1-21, on a 21-day cycle), Level B (doses 0.8 times A), or Level C (doses 0.6 times A). Alternatively, if the patient and clinician agreed the indication for chemotherapy was uncertain, the patient could instead enter CHEMO-BSC, comparing Level C vs best supportive care.
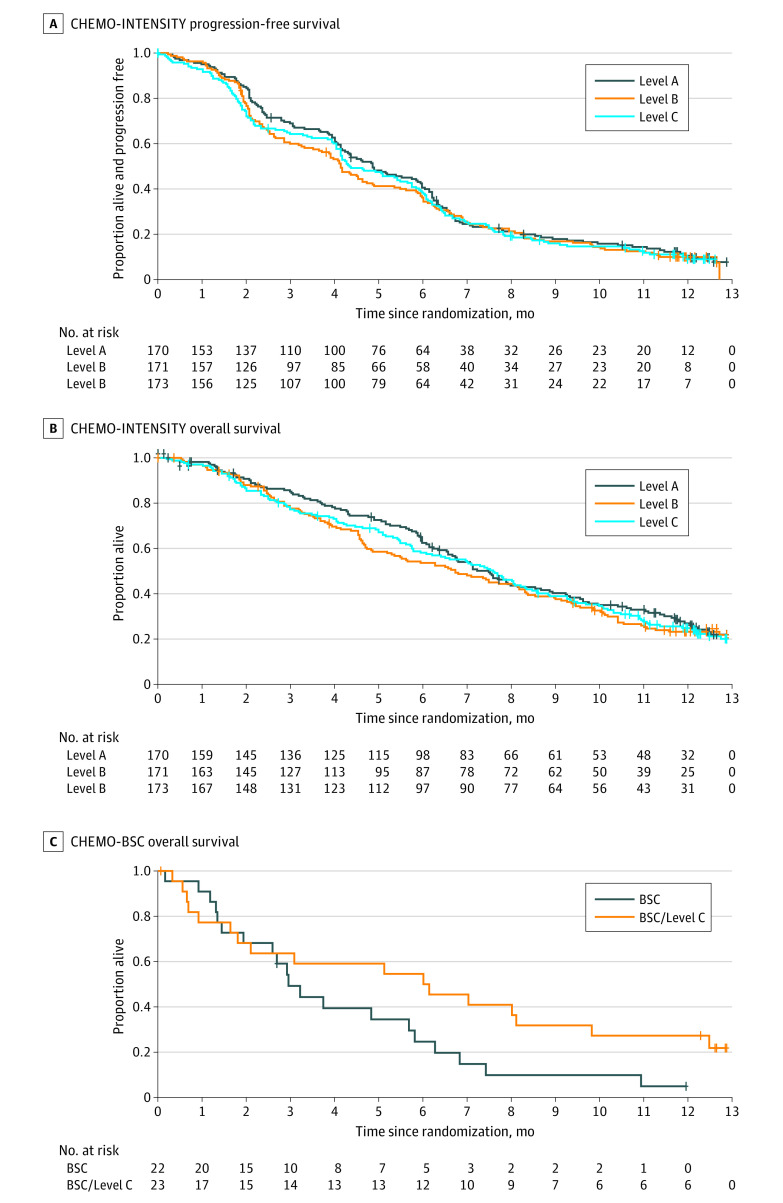
Main outcomes and measures: First, broad noninferiority of the lower doses vs reference (Level A) was assessed using a permissive boundary of 34 days reduction in progression-free survival (PFS) (hazard ratio, HR = 1.34), selected as acceptable by a forum of patients and clinicians. Then, the patient experience was compared using Overall Treatment Utility (OTU), which combines efficacy, toxic effects, quality of life, and patient value/acceptability. For CHEMO-BSC, the main outcome measure was overall survival.
Results: A total of 514 patients entered CHEMO-INTENSITY, of whom 385 (75%) were men and 299 (58%) were severely frail, with median age 76 years. Noninferior PFS was confirmed for Levels B vs A (HR = 1.09 [95% CI, 0.89-1.32]) and C vs A (HR = 1.10 [95% CI, 0.90-1.33]). Level C produced less toxic effects and better OTU than A or B. No subgroup benefited from higher doses: Level C produced better OTU even in younger or less frail patients. A total of 45 patients entered the CHEMO-BSC randomization: overall survival was nonsignificantly longer with chemotherapy: median 6.1 vs 3.0 months (HR = 0.69 [95% CI, 0.32-1.48], P = .34). In multivariate analysis in 522 patients with all variables available, baseline frailty, quality of life, and neutrophil to lymphocyte ratio were independently associated with OTU, and can be combined in a model to estimate the probability of different outcomes.
Conclusions and relevance: This phase 3 randomized clinical trial found that reduced-intensity chemotherapy provided a better patient experience without significantly compromising cancer control and should be considered for older and/or frail patients. Baseline geriatric assessment can help predict the utility of chemotherapy but did not identify a group benefiting from higher-dose treatment.
Trial registration: isrctn.org Identifier: ISRCTN44687907.
Conflict of interest statement
Figures
Comment in
-
Quantifying and Interpreting Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Cancer Control for Advanced Gastroesophageal Cancer Among an Older Population-Reply.JAMA Oncol. 2021 Nov 1;7(11):1725. doi: 10.1001/jamaoncol.2021.4010. JAMA Oncol. 2021. PMID: 34473203 No abstract available.
-
Quantifying and Interpreting Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Cancer Control for Advanced Gastroesophageal Cancer Among an Older Population.JAMA Oncol. 2021 Nov 1;7(11):1724-1725. doi: 10.1001/jamaoncol.2021.4007. JAMA Oncol. 2021. PMID: 34473208 No abstract available.
-
Quantifying and Interpreting Efficacy of Reduced-Intensity Chemotherapy With Oxaliplatin and Capecitabine on Cancer Control for Advanced Gastroesophageal Cancer Among an Older Population.JAMA Oncol. 2021 Nov 1;7(11):1723-1724. doi: 10.1001/jamaoncol.2021.4004. JAMA Oncol. 2021. PMID: 34473211 No abstract available.
References
-
- Al-Batran SE, Hartmann JT, Hofheinz R, et al. Biweekly fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) for patients with metastatic adenocarcinoma of the stomach or esophagogastric junction: a phase II trial of the Arbeitsgemeinschaft Internistische Onkologie. Ann Oncol. 2008;19(11):1882-1887. doi: 10.1093/annonc/mdn403 - DOI - PubMed
-
- Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. ; V325 Study Group . Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 Study Group. J Clin Oncol. 2006;24(31):4991-4997. doi: 10.1200/JCO.2006.06.8429 - DOI - PubMed
-
- Guimbaud R, Louvet C, Ries P, et al. Prospective, randomized, multicenter, phase III study of fluorouracil, leucovorin, and irinotecan versus epirubicin, cisplatin, and capecitabine in advanced gastric adenocarcinoma: a French intergroup (Fédération Francophone de Cancérologie Digestive, Fédération Nationale des Centres de Lutte Contre le Cancer, and Groupe Coopérateur Multidisciplinaire en Oncologie) study. J ClinOncol. 2014;32:3520-3526. doi: 10.1200/JCO.2013.54.1011 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
