

Virtual reality vs. Kalinox® for management of pain in intensive care unit after cardiac surgery: a randomized study
- PMID: 33983498
- PMCID: PMC8119554
- DOI: 10.1186/s13613-021-00866-w
Virtual reality vs. Kalinox® for management of pain in intensive care unit after cardiac surgery: a randomized study
Abstract
Introduction: The management of pain and anxiety remains a challenge in the intensive care unit. By distracting patients, virtual reality (VR) may have a role in painful procedures. We compared VR vs. an inhaled equimolar mixture of N2O and O2 (Kalinox®) for pain and anxiety management during the removal of chest drains after cardiac surgery.
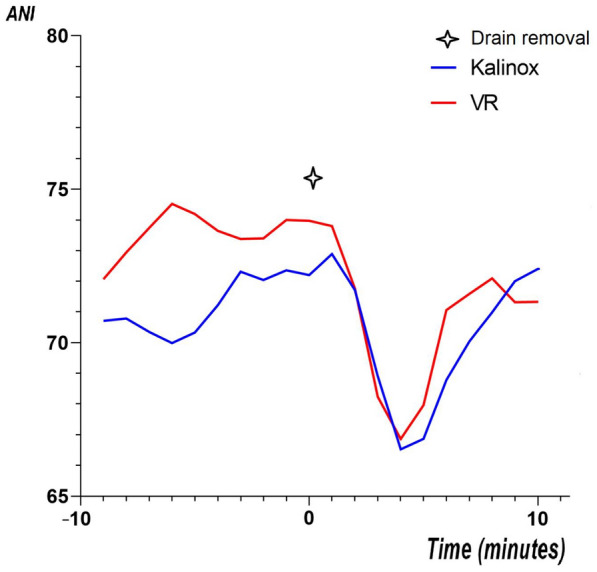
Methods: Prospective, non-inferiority, open-label study. Patients were randomized, for Kalinox® or VR session during drain removal. The analgesia/nociception index (ANI) was monitored during the procedure for objective assessment of pain and anxiety. The primary endpoint was the ΔANI (ANImin - ANI0) during the procedure, based on ANIm (average on 4 min). We prespecified VR as non-inferior to Kalinox® with a margin of 3 points. Self-reported pain and anxiety were also analysed using numeric rate scale (NRS).
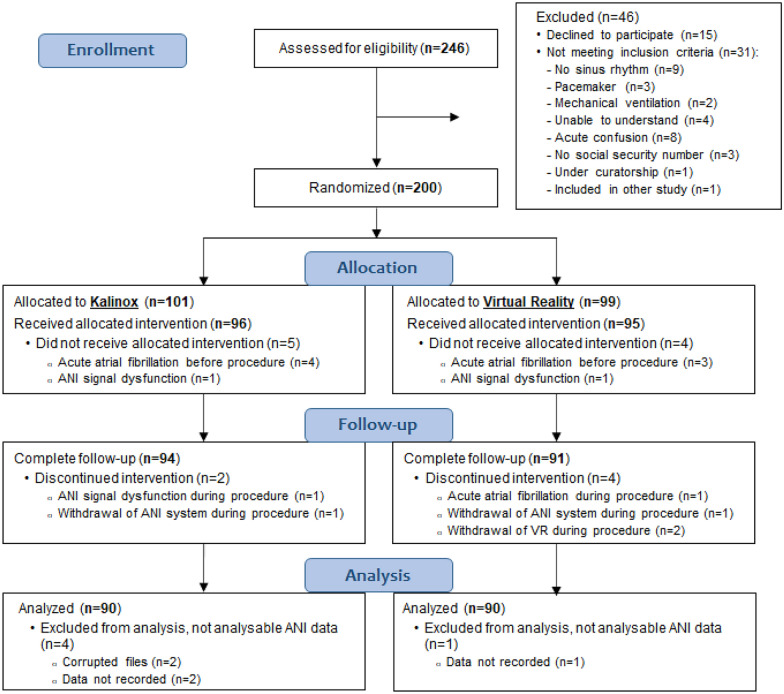
Results: 200 patients were included, 99 in the VR group and 101 in the Kalinox® group; 90 patients were analysed in both groups in per-protocol analysis. The median age was 68.0 years [60.0-74.8]. The ΔANI was - 15.1 ± 12.9 in the Kalinox® group and - 15.7 ± 11.6 in the VR group (NS). The mean difference was, therefore, - 0.6 [- 3.6 to 2.4], including the non-inferiority margin of 3. Patients in the VR group had a significantly higher pain NRS scale immediately after the drain removal, 5.0 [3.0-7.0] vs. 3.0 [2.0-6.0], p = 0.009, but no difference 10 min after. NRS of anxiety did not differ between the two groups.
Conclusion: Based on the ANI, the current study showed that VR did not reach the statistical requirements for a proven non-inferiority vs. Kalinox® in managing pain and anxiety during chest drain removal. Moreover, VR was less effective based on NRS. More studies are needed to determine if VR might have a place in the overall approach to pain and anxiety in intensive care units. Trial registration NCT, NCT03956264. Registered 20 May 2019, https://clinicaltrials.gov/ct2/show/NCT03956264.
Keywords: Analgesia; Cardiac surgery; Kalinox®; Perioperative pain; Virtual reality.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Puntillo KA, Max A, Timsit JF, Vignoud L, Chanques G, Robleda G, et al. Determinants of procedural pain intensity in the intensive care unit. The Europain® study. Am J Respir Crit Care Med. 2014;189(1):39–47. - PubMed
-
- Gift AG, Bolgiano CS, Cunningham J. Sensations during chest tube removal. Heart Lung. 1991;20(2):131–137. - PubMed
-
- Schelling G, Richter M, Roozendaal B, Rothenhäusler HB, Krauseneck T, Stoll C, et al. Exposure to high stress in the intensive care unit may have negative effects on health-related quality-of-life outcomes after cardiac surgery. Crit Care Med. 2003;31(7):1971–1980. doi: 10.1097/01.CCM.0000069512.10544.40. - DOI - PubMed
-
- Carson MM, Barton DM, Morrison CC, Tribble CG. Managing pain during mediastinal chest tube removal. Heart Lung. 1994;23(6):500–505. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
