

Assessment of the causal relevance of ECG parameters for risk of atrial fibrillation: A mendelian randomisation study
- PMID: 33983917
- PMCID: PMC8118296
- DOI: 10.1371/journal.pmed.1003572
Assessment of the causal relevance of ECG parameters for risk of atrial fibrillation: A mendelian randomisation study
Abstract
Background: Atrial electrical and structural remodelling in older individuals with cardiovascular risk factors has been associated with changes in surface electrocardiographic (ECG) parameters (e.g., prolongation of the PR interval) and higher risks of atrial fibrillation (AF). However, it has been difficult to establish whether altered ECG parameters are the cause or a consequence of the myocardial substrate leading to AF. This study aimed to examine the potential causal relevance of ECG parameters on risk of AF using mendelian randomisation (MR).
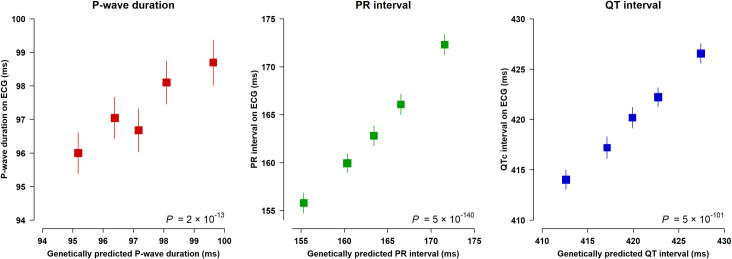
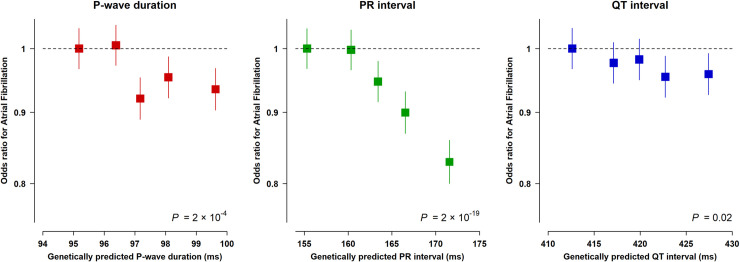
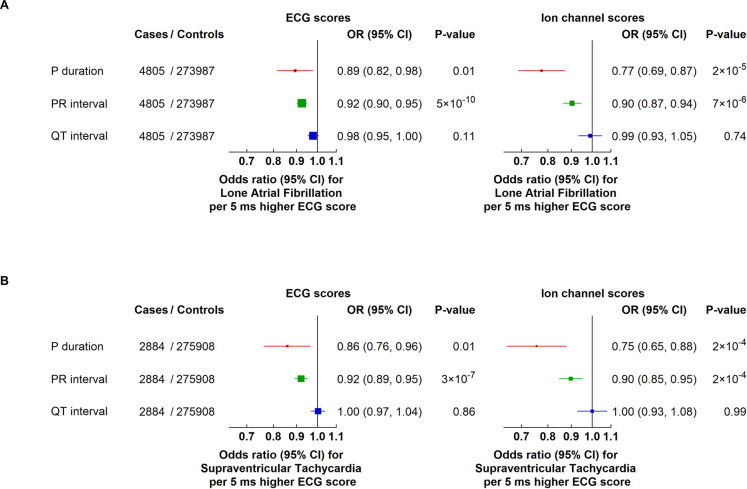
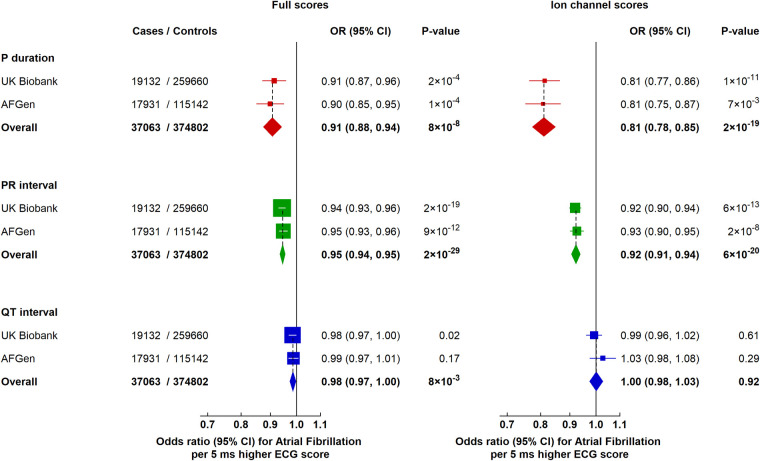
Methods and findings: Weighted genetic scores explaining lifelong differences in P-wave duration, PR interval, and QT interval were constructed, and associations between these ECG scores and risk of AF were estimated among 278,792 UK Biobank participants (mean age: 57 years at recruitment; 19,132 AF cases). The independent genetic variants contributing to each of the separate ECG scores, and their corresponding weights, were based on published genome-wide association studies. In UK Biobank, genetic scores representing a 5 ms longer P-wave duration or PR interval were significantly associated with lower risks of AF (odds ratio [OR] 0.91; 95% confidence interval [CI]: 0.87-0.96, P = 2 × 10-4 and OR 0.94; 95% CI: 0.93-0.96, P = 2 × 10-19, respectively), while longer QT interval was not significantly associated with AF. These effects were independently replicated among a further 17,931 AF cases from the AFGen Consortium. Investigation of potential mechanistic pathways showed that differences in ECG parameters associated with specific ion channel genes had effects on risk of AF consistent with the overall scores, while the overall scores were not associated with changes in left atrial size. Limitations of the study included the inherent assumptions of MR, restriction to individuals of European ancestry, and possible restriction of results to the normal ECG ranges represented in UK Biobank.
Conclusions: In UK Biobank, we observed evidence suggesting a causal relationship between lifelong differences in ECG parameters (particularly PR interval) that reflect longer atrial conduction times and a lower risk of AF. These findings, which appear to be independent of atrial size and concomitant cardiovascular comorbidity, support the relevance of varying mechanisms underpinning AF and indicate that more individualised treatment strategies warrant consideration.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: PRG, AVE, MI, EVM, CFC, FM, AS and JCH work at the Clinical Trial Service Unit & Epidemiological Studies Unit, Nuffield Department of Population Health, which receives research grants from industry that are governed by University of Oxford contracts that protect its independence, and has a staff policy of not taking personal payments from industry; further details can be found at https://www.ndph.ox.ac.uk/files/about/ndph-independence-of-research-policy-jun-20.pdf. BC is supported by a British Heart Foundation (BHF) personal chair; her research is funded by two BHF Programme Grants, the BHF Centre for Research Excellence and the NIHR Oxford Biomedical Research Centre. She also receives in-kind research support from iRhythm and Roche Diagnostics. JCH is supported by a British Heart Foundation personal Fellowship; her research is also funded by grants from industry held in accordance with the policy detailed above, and the Nuffield Department of Population Health.
Figures
Similar articles
-
Sex hormones and reproductive factors with cardiac arrhythmia and ECG indices: a mendelian randomization study.BMC Cardiovasc Disord. 2024 Nov 20;24(1):659. doi: 10.1186/s12872-024-04335-7. BMC Cardiovasc Disord. 2024. PMID: 39567890 Free PMC article.
-
Heart rate variability and atrial fibrillation in the general population: a longitudinal and Mendelian randomization study.Clin Res Cardiol. 2023 Jun;112(6):747-758. doi: 10.1007/s00392-022-02072-5. Epub 2022 Aug 13. Clin Res Cardiol. 2023. PMID: 35962833 Free PMC article.
-
Exploring the causal association of rheumatoid arthritis with atrial fibrillation: a Mendelian randomization study.Clin Rheumatol. 2024 Jan;43(1):29-40. doi: 10.1007/s10067-023-06804-4. Epub 2023 Nov 6. Clin Rheumatol. 2024. PMID: 37930596
-
Exploring the causal relationships and mediating factors between depression, anxiety, panic, and atrial fibrillation: A multivariable Mendelian randomization study.J Affect Disord. 2024 Mar 15;349:635-645. doi: 10.1016/j.jad.2024.01.061. Epub 2024 Jan 9. J Affect Disord. 2024. PMID: 38211754
-
Analysing electrocardiographic traits and predicting cardiac risk in UK biobank.JRSM Cardiovasc Dis. 2021 Jun 12;10:20480040211023664. doi: 10.1177/20480040211023664. eCollection 2021 Jan-Dec. JRSM Cardiovasc Dis. 2021. PMID: 34211707 Free PMC article. Review.
Cited by
-
Dissecting the causal effects of smoking, alcohol consumption, and related DNA methylation markers on electrocardiographic indices.Clin Epigenetics. 2025 Mar 4;17(1):40. doi: 10.1186/s13148-025-01851-x. Clin Epigenetics. 2025. PMID: 40038836 Free PMC article.
-
A Nomogram utilizing ECG P-wave parameters to predict recurrence risk following catheter ablation in paroxysmal atrial fibrillation.J Cardiothorac Surg. 2025 Jan 25;20(1):94. doi: 10.1186/s13019-024-03335-0. J Cardiothorac Surg. 2025. PMID: 39863909 Free PMC article.
-
Causal Relationship Between Electrocardiogram Parameters and Brugada Syndrome: A Bidirectional Mendelian Randomization Study.Ann Noninvasive Electrocardiol. 2025 Mar;30(2):e70060. doi: 10.1111/anec.70060. Ann Noninvasive Electrocardiol. 2025. PMID: 40070266 Free PMC article.
-
Genetic and phenotypic associations of frailty with cardiovascular indicators and behavioral characteristics.J Adv Res. 2025 May;71:263-277. doi: 10.1016/j.jare.2024.06.012. Epub 2024 Jun 9. J Adv Res. 2025. PMID: 38862035 Free PMC article.
-
[Intrinsic steady-state pattern of mouse cardiac electrophysiology: analysis using a characterized quantitative electrocardiogram strategy].Nan Fang Yi Ke Da Xue Xue Bao. 2024 Oct 20;44(10):1985-1994. doi: 10.12122/j.issn.1673-4254.2024.10.17. Nan Fang Yi Ke Da Xue Xue Bao. 2024. PMID: 39523099 Free PMC article. Chinese.
References
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr, et al.. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125–e51. 10.1161/CIR.0000000000000665 . - DOI - PubMed
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al.. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373–498. 10.1093/eurheartj/ehaa612 . - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- 16896/CRUK_/Cancer Research UK/United Kingdom
- RG/18/6/33576/BHF_/British Heart Foundation/United Kingdom
- FS/17/17/32438 /BHF_/British Heart Foundation/United Kingdom
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- FS/20/15/34920/BHF_/British Heart Foundation/United Kingdom
- DH_/Department of Health/United Kingdom
- FS/17/17/32438/BHF_/British Heart Foundation/United Kingdom
- FS/14/55/30806/BHF_/British Heart Foundation/United Kingdom
- FS/14/55/30806/BHF_/British Heart Foundation/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- FS/20/15/34920/BHF_/British Heart Foundation/United Kingdom
- CH/12/3/29609/BHF_/British Heart Foundation/United Kingdom
- RG/16/12/3245/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
