

Quantitative assessment of lung involvement on chest CT at admission: Impact on hypoxia and outcome in COVID-19 patients
- PMID: 33984670
- PMCID: PMC8081746
- DOI: 10.1016/j.clinimag.2021.04.033
Quantitative assessment of lung involvement on chest CT at admission: Impact on hypoxia and outcome in COVID-19 patients
Abstract
Background: The aim of this study was to quantify COVID-19 pneumonia features using CT performed at time of admission to emergency department in order to predict patients' hypoxia during the hospitalization and outcome.
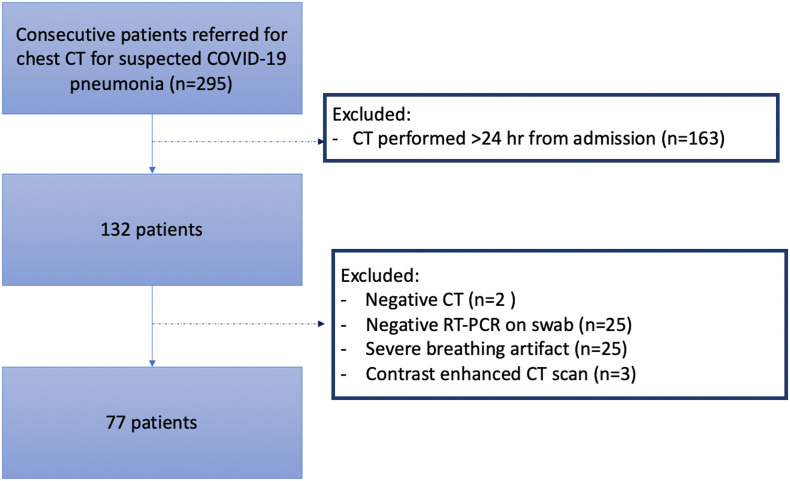
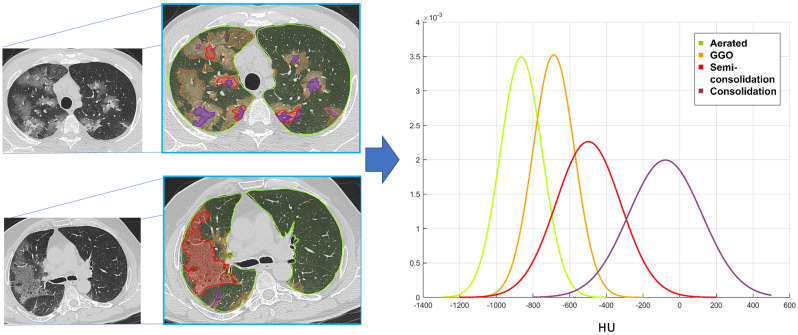
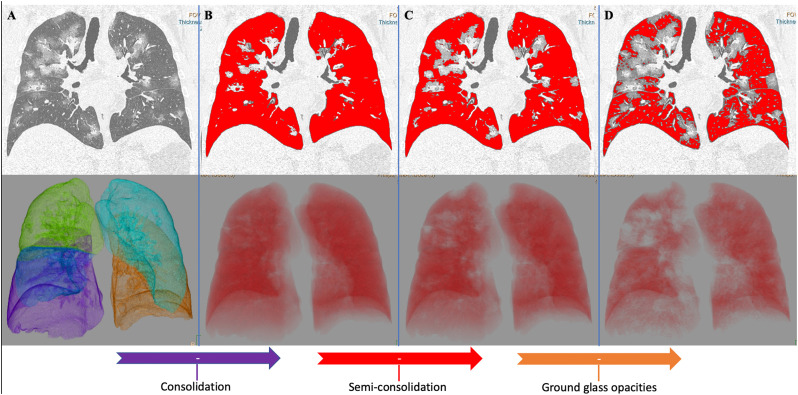
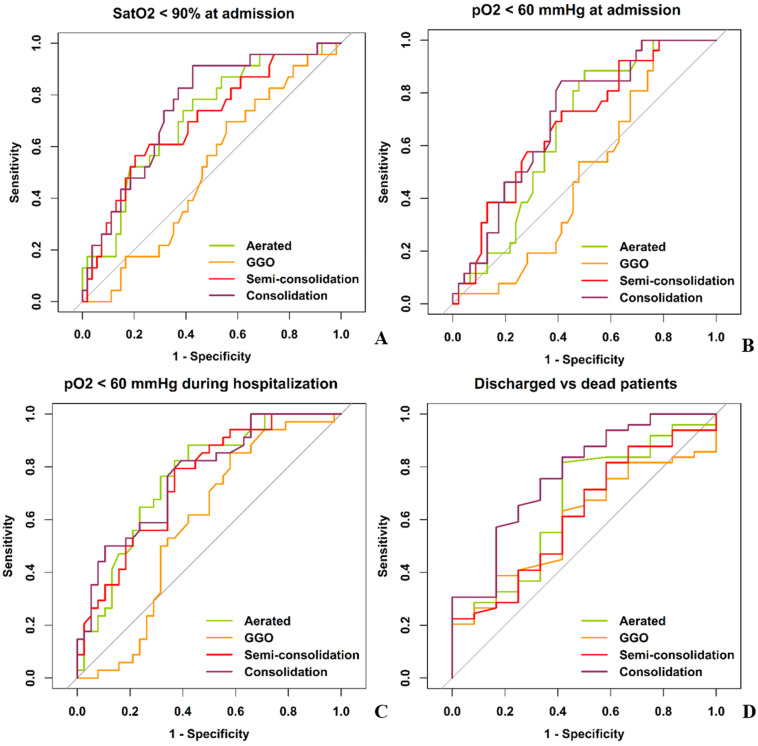
Methods: Consecutive chest CT performed in the emergency department between March 1st and April 7th 2020 for COVID-19 pneumonia were analyzed. The three features of pneumonia (GGO, semi-consolidation and consolidation) and the percentage of well-aerated lung were quantified using a HU threshold based software. ROC curves identified the optimal cut-off values of CT parameters to predict hypoxia worsening and hospital discharge. Multiple Cox proportional hazards regression was used to analyze the capability of CT quantitative features, demographic and clinical variables to predict the time to hospital discharge.
Results: Seventy-seven patients (median age 56-years-old, 51 men) with COVID-19 pneumonia at CT were enrolled. The quantitative features of COVID-19 pneumonia were not associated to age, sex and time-from-symptoms onset, whereas higher number of comorbidities was correlated to lower well-aerated parenchyma ratio (rho = -0.234, p = 0.04) and increased semi-consolidation ratio (rho = -0.303, p = 0.008). Well-aerated lung (≤57%), semi-consolidation (≥17%) and consolidation (≥9%) predicted worst hypoxemia during hospitalization, with moderate areas under curves (AUC 0.76, 0.75, 0.77, respectively). Multiple Cox regression identified younger age (p < 0.01), female sex (p < 0.001), longer time-from-symptoms onset (p = 0.049), semi-consolidation ≤17% (p < 0.01) and consolidation ≤13% (p = 0.03) as independent predictors of shorter time to hospital discharge.
Conclusion: Quantification of pneumonia features on admitting chest CT predicted hypoxia worsening during hospitalization and time to hospital discharge in COVID-19 patients.
Keywords: Artificial intelligence; Covid-19; Outcome; Pneumonia; Quantitative CT.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Simpson S., Kay F.U., Abbara S., et al. Radiological society of North America expert consensus document on reporting chest CT findings related to COVID-19: endorsed by the society of thoracic radiology, the American college of radiology, and RSNA. Radiol Cardiothoracic Imag. 2020 Mar 25;2(2) - PMC - PubMed
-
- Remy-Jardin M., Giraud F., Remy J., Copin M.C., Gosselin B., Duhamel A. Importance of ground-glass attenuation in chronic diffuse infiltrative lung disease: pathologic-CT correlation. Radiology. 1993 Dec;189(3):693–698. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
