

High BRAF variant allele frequencies are associated with distinct pathological features and responsiveness to target therapy in melanoma patients
- PMID: 33984673
- PMCID: PMC8134716
- DOI: 10.1016/j.esmoop.2021.100133
High BRAF variant allele frequencies are associated with distinct pathological features and responsiveness to target therapy in melanoma patients
Abstract
Background: BRAF mutant melanoma patients are commonly treated with anti-BRAF therapeutic strategies. However, many factors, including the percentage of BRAF-mutated cells, may contribute to the great variability in patient outcomes.
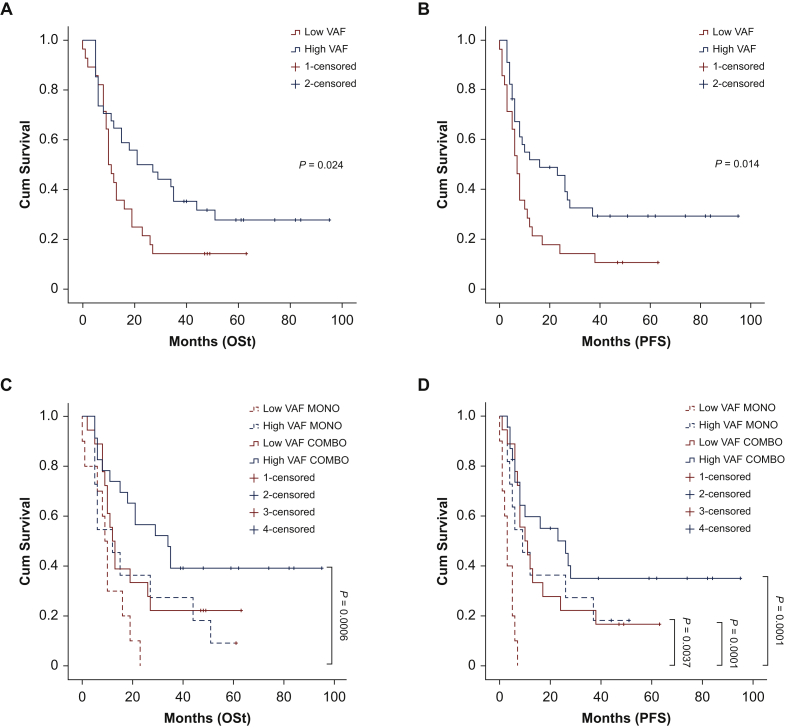
Patients and methods: The BRAF variant allele frequency (VAF; defined as the percentage of mutated alleles) of primary and secondary melanoma lesions, obtained from 327 patients with different disease stages, was assessed by pyrosequencing. The BRAF mutation rate and VAF were then correlated with melanoma pathological features and patients' clinical characteristics. Kaplan-Meier curves were used to study the correlations between BRAF VAF, overall survival (OS), and progression-free survival (PFS) in a subset of 62 patients treated by anti-BRAF/anti-MEK therapy after metastatic progression.
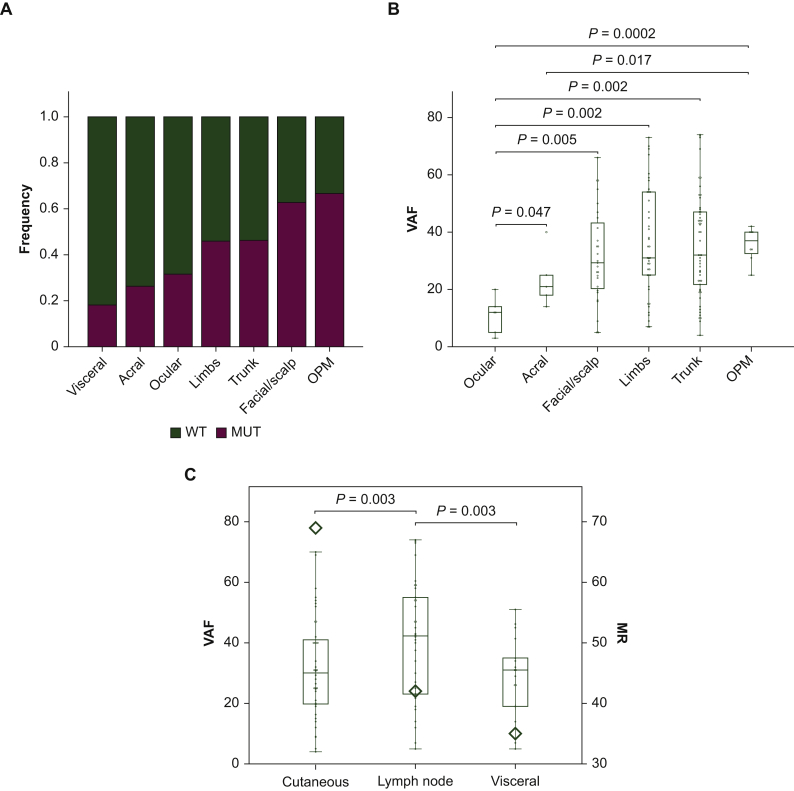
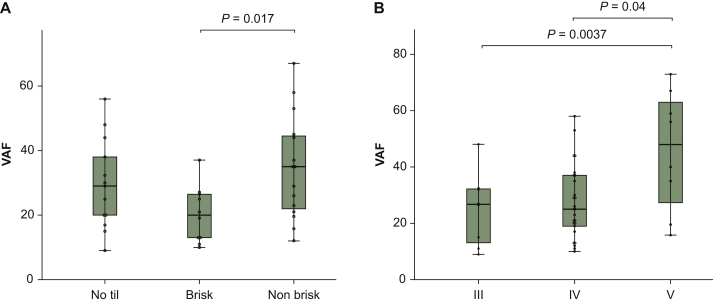
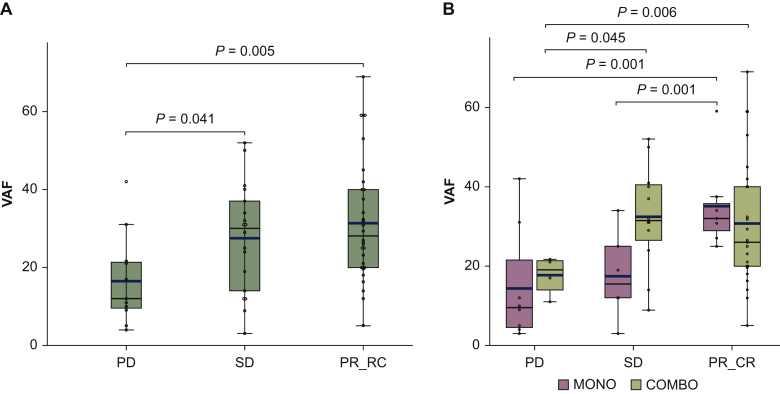
Results: A highly heterogeneous BRAF VAF was identified (3%-90%). Besides being correlated with age, a higher BRAF VAF level was related to moderate lymphocytic infiltration (P = 0.017), to melanoma thickness according to Clark levels, (level V versus III, P = 0.004; level V versus IV, P = 0.04), to lymph node metastases rather than cutaneous (P = 0.04) or visceral (P = 0.03) secondary lesions. In particular, a BRAF VAF >25% was significantly associated with a favorable outcome in patients treated with the combination of anti-BRAF/anti-MEK drug (OS P = 0.04; PFS P = 0.019), retaining a significant value as an independent factor for the OS and the PFS in the multivariate analysis (P = 0.014 and P = 0.003, respectively).
Conclusion: These results definitively support the role of the BRAF VAF as a potential prognostic and predictive biomarker in melanoma patients in the context of BRAF inhibition.
Keywords: BRAF mutations; increased survival; melanoma; variant allele frequency.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure The authors have declared no conflicts of interest. Data sharing All data relevant to the study are included in the article or uploaded as online supplemental information. Individual patient data cannot be shared. Disclaimer The views expressed are those of the author(s) and not necessarily those of the Candiolo Cancer Institute or the University of Turin. Ethics approval Clinical-pathological data were recovered after obtaining the informed consent from all the patients, approved by the medical ethical committee of the FPO-IRCCS, and carried out according to the principles of the Declaration of Helsinki.
Figures
References
-
- Society AC A.C. Cancer Facts & Figures 2019. 2019. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-... Cited 2018. Available at.
-
- Davies H., Bignell G.R., Cox C. Mutations of the BRAF gene in human cancer. Nature. 2002;417(6892):949–954. - PubMed
-
- Omholt K., Platz A., Kanter L. NRAS and BRAF mutations arise early during melanoma pathogenesis and are preserved throughout tumor progression. Clin Cancer Res. 2003;9(17):6483–6488. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
