

Lack of prognostic impact of sentinel node micro-metastases in endocrine receptor-positive early breast cancer: results from a large multicenter cohort☆
- PMID: 33984674
- PMCID: PMC8314870
- DOI: 10.1016/j.esmoop.2021.100151
Lack of prognostic impact of sentinel node micro-metastases in endocrine receptor-positive early breast cancer: results from a large multicenter cohort☆
Abstract
Background: Prognostic impact of lymph node micro-metastases (pN1mi) has been discordantly reported in the literature. The need to clarify this point for decision-making regarding adjuvant therapy, particularly for patients with endocrine receptor (ER)-positive status and HER2-negative tumors, is further reinforced by the generalization of gene expression signatures using pN status in their recommendation algorithm.
Patients and methods: We retrospectively analyzed 13 773 patients treated for ER-positive breast cancer in 13 French cancer centers from 1999 to 2014. Five categories of axillary lymph node (LN) status were defined: negative LN (pN0i-), isolated tumor cells [pN0(i+)], pN1mi, and pN1 divided into single (pN1 = 1) and multiple (pN1 > 1) macro-metastases (>2 mm). The effect of LN micro-metastases on outcomes was investigated both in the entire cohort of patients and in clinically relevant subgroups according to tumor subtypes. Propensity-score-based matching was used to balance differences in known prognostic variables associated with pN status.
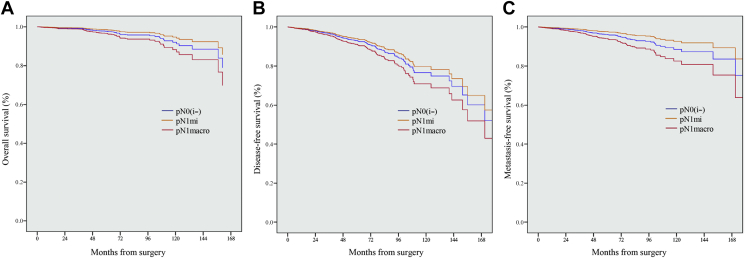
Results: As determined by sentinel LN biopsy, 9427 patients were pN0 (68.4%), 546 pN0(i+) (4.0%), 1446 pN1mi (10.5%) and 2354 pN1 with macro-metastases (17.1%). With a median follow-up of 61.25 months, pN1 status, but not pN1mi, significantly impacted overall survival (OS), disease-free survival (DFS), metastasis-free survival (MFS), and breast-cancer-specific survival. In the subgroup of patients with known tumor subtype, pN1 = 1, as pN1 > 1, but not pN1mi, had a significant prognostic impact on OS. DFS and MFS were only impacted by pN1 > 1. Similar results were observed in the subgroup of patients with luminal A-like tumors (n = 7101). In the matched population analysis, pN1macro, but not pN1mi, had a statistically significant negative impact on MFS and OS.
Conclusion: LN micro-metastases have no detectable prognostic impact and should not be considered as a determining factor in indicating adjuvant chemotherapy. The evaluation of the risk of recurrence using second-generation signatures should be calculated considering micro-metastases as pN0.
Trial registration: ClinicalTrials.gov NCT02869607.
Keywords: breast cancer; micro-metastases; sentinel node; survival.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure The authors have declared no conflicts of interest. Data sharing The data sets generated and/or analyzed during the current study are not publicly available, as the study has used clinical databases of 13 different comprehensive cancer centers in France (ClinicalTrials.govNCT02869607).
Figures





References
-
- Burstein H.J., Curigliano G., Loibl S. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541–1557. - PubMed
-
- Schwartz A.M., Henson D.E., Chen D., Rajamarthandan S. Histologic grade remains a prognostic factor for breast cancer regardless of the number of positive lymph nodes and tumor size: a study of 161 708 cases of breast cancer from the SEER program. Arch Pathol Lab Med. 2014;138(8):1048–1052. - PubMed
-
- Mohammed R.A.A., Martin S.G., Gill M.S., Green A.R., Paish E.C., Ellis I.O. Improved methods of detection of lymphovascular invasion demonstrate that it is the predominant method of vascular invasion in breast cancer and has important clinical consequences. Am J Surg Pathol. 2007;31(12):1825–1833. - PubMed
-
- Cianfrocca M. Prognostic and predictive factors in early-stage breast cancer. Oncologist. 2004;9(6):606–616. - PubMed
-
- Jafferbhoy S., McWilliams B. Clinical significance and management of sentinel node micrometastasis in invasive breast cancer. Clin Breast Cancer. 2012;12(5):308–312. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
