

Evaluation of uterine scar healing by transvaginal ultrasound in 607 nonpregnant women with a history of cesarean section
- PMID: 33985487
- PMCID: PMC8117607
- DOI: 10.1186/s12905-021-01337-x
Evaluation of uterine scar healing by transvaginal ultrasound in 607 nonpregnant women with a history of cesarean section
Abstract
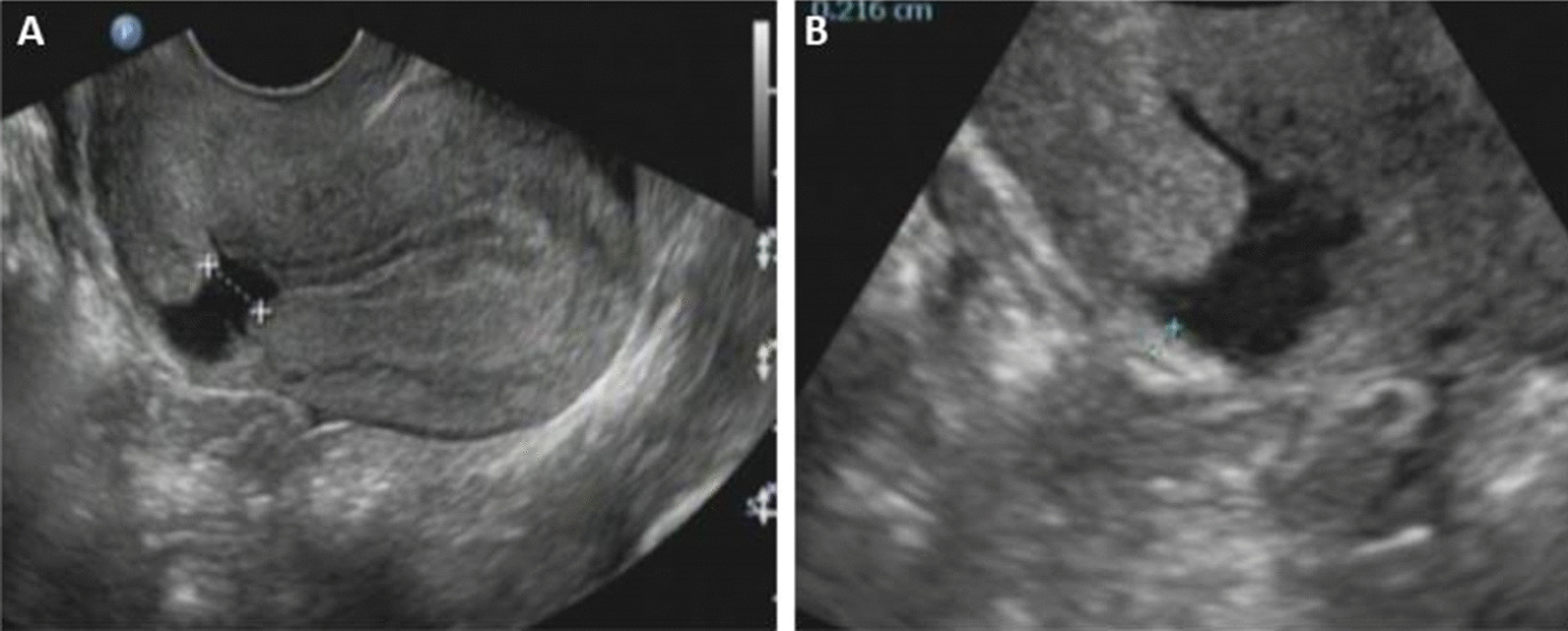
Background: Caesarean scar defect (CSD) seriously affects female reproductive health. In this study, we aim to evaluate uterine scar healing by transvaginal ultrasound (TVS) in nonpregnant women with cesarean section (CS) history and to build a predictive model for cesarean scar defects is very necessary.
Methods: A total of 607 nonpregnant women with previous CS who have transvaginal ultrasound measurements of the thickness of the lower uterine segment. The related clinical data were recorded and analyzed.
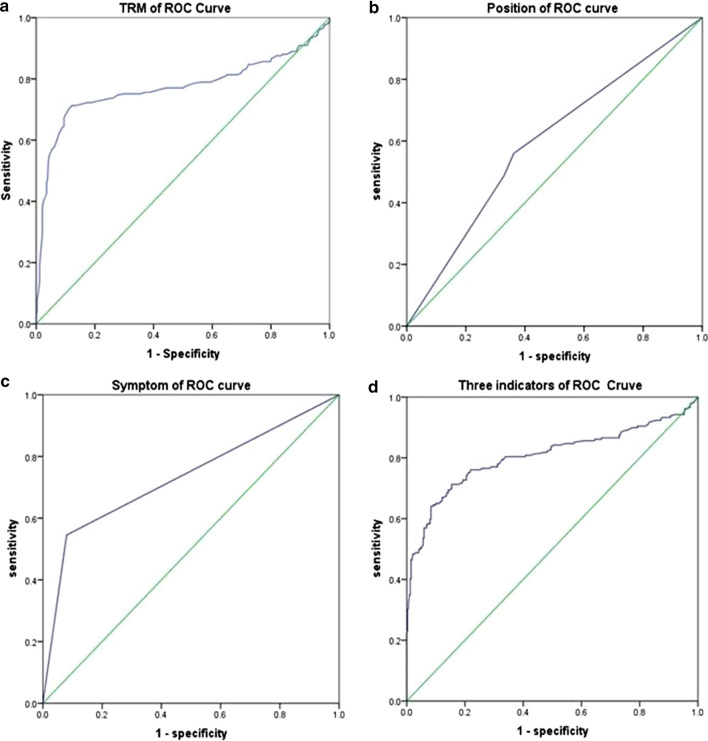
Results: All patients were divided into two groups according to their clinical symptoms: Group A (N = 405) who had no cesarean scar symptoms, and Group B (N = 141) who had cesarean scar symptoms. The difference in frequency of CS, uterine position, detection rate of CSD and the residual muscular layer (TRM) of the CSD were statistically significant between groups; the TRM measurements of the two groups were (mm) 5.39 ± 3.34 versus 3.22 ± 2.33, P < 0.05. All patients were divided into two groups according to whether they had CSDs: Group C (N = 337) who had no CSDs, Group D (N = 209) who had CSDs on ultrasound examination. The differences in frequency of CS, uterine position, TRM between groups were statistically significant (P < 0.05). In the model predicting CSDs by TRM with TVS, the area under the ROC curve was 0.771, the cut-off value was 4.15 mm. The sensitivity and specificity were 87.8% and 71.3%, respectively.
Conclusions: Patients with no clinical symptoms had a mean TRM on transvaginal ultrasonography of 5.39 ± 3.34 mm, which could be used as a good reference to predict the recovery of patients with CSDs after repair surgery.
Keywords: Cesarean scar defect (CSD); Cesarean section; Predictive model; Thickness of residual myometrial (TRM); Transvaginal ultrasound (TVS).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bij de Vaate AJ, van der Voet LF, Naji O, Witmer M, Veersema S, Brolmann HA, et al. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound Obstet Gynecol. 2014;43(4):372–382. doi: 10.1002/uog.13199. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
