

Factors Predisposing to Survival After Resuscitation for Sudden Cardiac Arrest
- PMID: 33985679
- PMCID: PMC8167892
- DOI: 10.1016/j.jacc.2021.03.299
Factors Predisposing to Survival After Resuscitation for Sudden Cardiac Arrest
Abstract
Background: In the POST SCD study, the authors autopsied all World Health Organization (WHO)-defined sudden cardiac deaths (SCDs) and found that only 56% had an arrhythmic cause; resuscitated sudden cardiac arrests (SCAs) were excluded because they did not die suddenly. They hypothesized that causes underlying resuscitated SCAs would be similarly heterogeneous.
Objectives: The aim of this study was to determine the causes and outcomes of resuscitated SCAs.
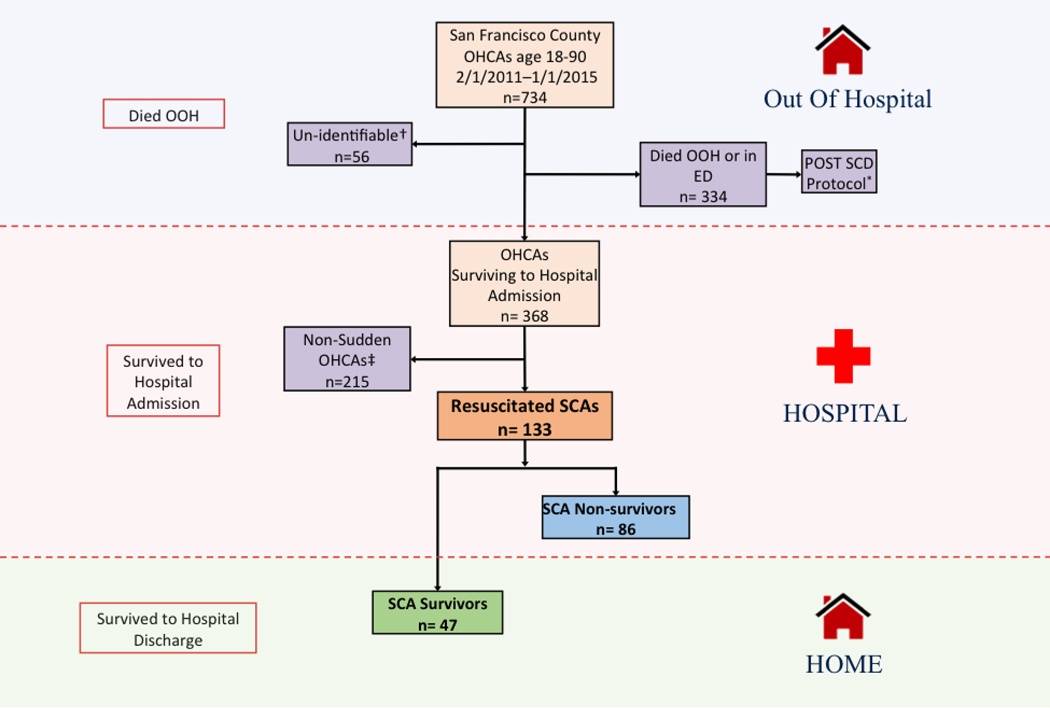
Methods: The authors identified all out-of-hospital cardiac arrests (OHCAs) from February 1, 2011, to January 1, 2015, of patients aged 18 to 90 years in San Francisco County. Resuscitated SCAs were OHCAs surviving to hospitalization and meeting WHO criteria for suddenness. Underlying cause was determined by comprehensive record review.
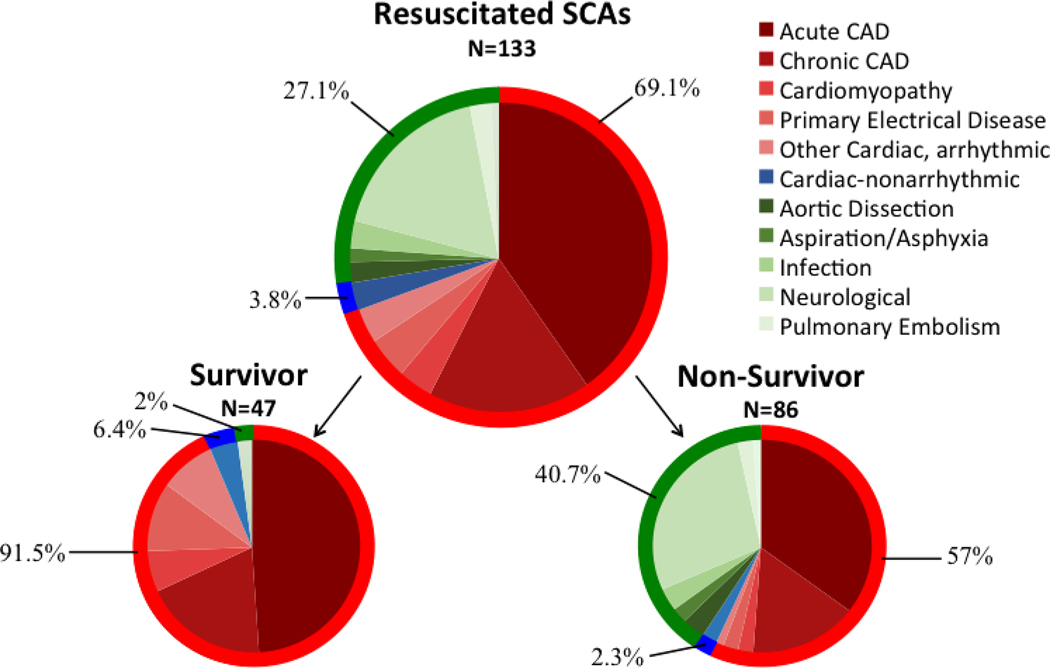
Results: The authors identified 734 OHCAs over 48 months; 239 met SCA criteria, 133 (55.6%) were resuscitated to hospitalization, and 47 (19.7%) survived to discharge. Arrhythmic causes accounted for significantly more resuscitated SCAs overall (92 of 133, 69.1%), particularly among survivors (43 of 47, 91.5%), than WHO-defined SCDs in POST SCD (293 of 525, 55.8%; p < 0.004 for both). Among resuscitated SCAs, arrhythmic cause, ventricular tachycardia/fibrillation initial rhythm, and white race were independent predictors of survival. None of the resuscitated SCAs due to neurologic causes survived.
Conclusions: In this 4-year countywide study of OHCAs, only one-third were sudden, of which one-half were resuscitated to hospitalization and 1 in 5 survived to discharge. Arrhythmic cause predicted survival and nearly one-half of nonsurvivors had nonarrhythmic causes, suggesting that SCA survivors are not equivalent to SCDs. Early identification of nonarrhythmic SCAs, such as neurologic emergencies, may be a target to improve OHCA survival.
Keywords: out of hospital cardiac arrest; resuscitation; sudden cardiac death.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was funded by the National Institutes of Health (NIH) National Heart, Lung, and Blood Institute (NHLBI) (R01 HL102090 to Dr. Tseng). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. Dr. Tseng has received grants from NIH/NHLBI and the Centers for Disease Control and Prevention during the conduct of the study, and personal fees from Biotronik outside the submitted work. Dr. Salazar has received a grant (R38HL143581) from the NHLBI. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
The Shadows of Sudden Cardiac Death.J Am Coll Cardiol. 2021 May 18;77(19):2363-2365. doi: 10.1016/j.jacc.2021.03.321. J Am Coll Cardiol. 2021. PMID: 33985680 No abstract available.
-
Sudden Death: Thinking Beyond the Heart.J Am Coll Cardiol. 2021 Sep 7;78(10):e61. doi: 10.1016/j.jacc.2021.06.046. J Am Coll Cardiol. 2021. PMID: 34474742 No abstract available.
-
Reply: Sudden Death: Thinking Beyond the Heart.J Am Coll Cardiol. 2021 Sep 7;78(10):e63. doi: 10.1016/j.jacc.2021.07.007. J Am Coll Cardiol. 2021. PMID: 34474743 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
