

Impact of Major Residual Lesions on Outcomes After Surgery for Congenital Heart Disease
- PMID: 33985683
- PMCID: PMC8245007
- DOI: 10.1016/j.jacc.2021.03.304
Impact of Major Residual Lesions on Outcomes After Surgery for Congenital Heart Disease
Abstract
Background: Many factors affect outcomes after congenital cardiac surgery.
Objectives: The RLS (Residual Lesion Score) study explored the impact of severity of residual lesions on post-operative outcomes across operations of varying complexity.
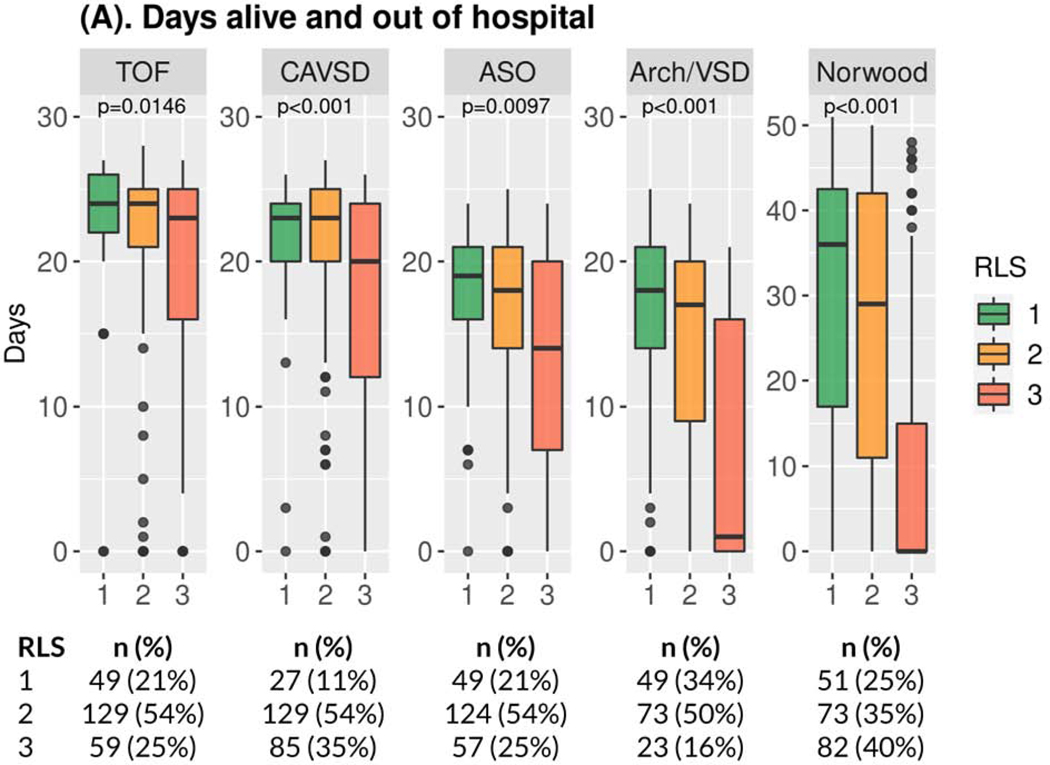
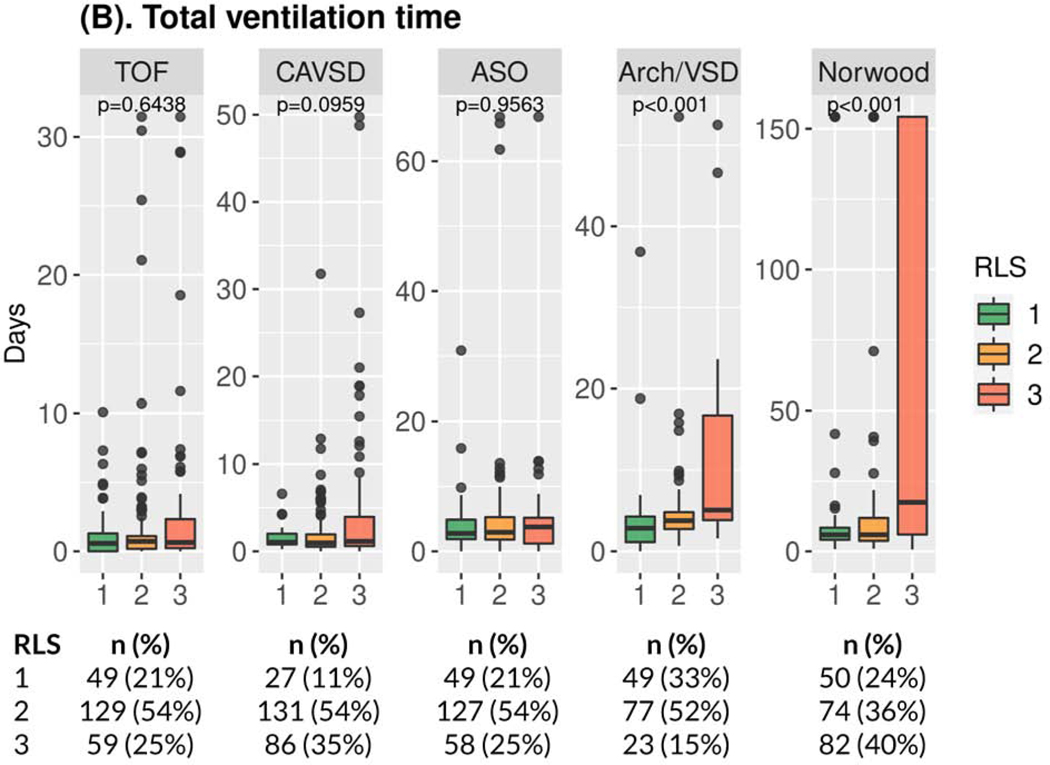
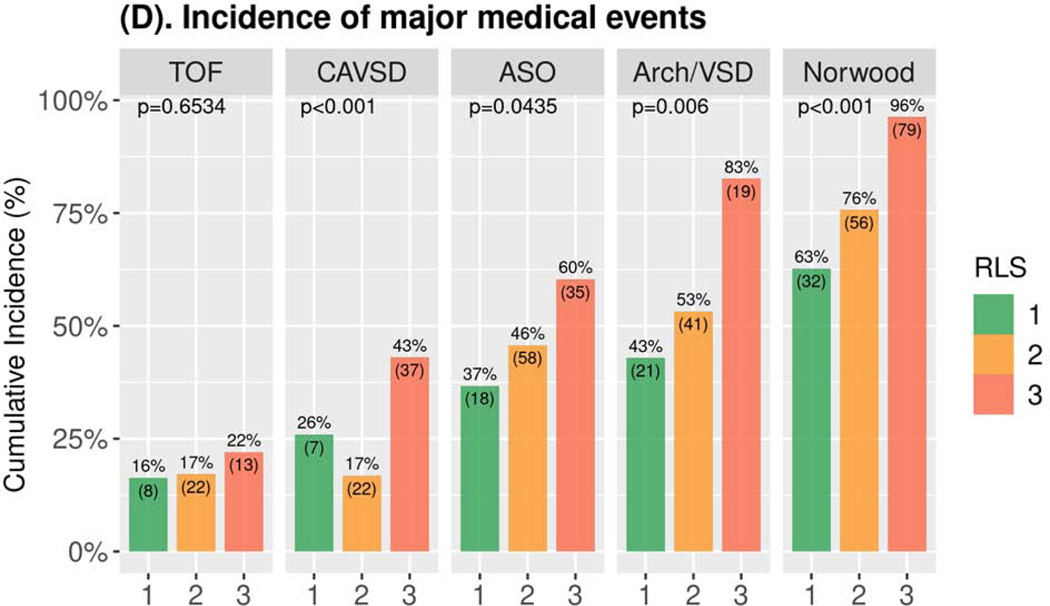
Methods: In a prospective, multicenter, observational study, 17 sites enrolled 1,149 infants undergoing 5 common operations: tetralogy of Fallot repair (n = 250), complete atrioventricular septal defect repair (n = 249), arterial switch operation (n = 251), coarctation or interrupted arch with ventricular septal defect (VSD) repair (n = 150), and Norwood operation (n = 249). The RLS was assigned based on post-operative echocardiography and clinical events: RLS 1 (trivial or no residual lesions), RLS 2 (minor residual lesions), or RLS 3 (reintervention for or major residual lesions before discharge). The primary outcome was days alive and out of hospital within 30 post-operative days (60 for Norwood). Secondary outcomes assessed post-operative course, including major medical events and days in hospital.
Results: RLS 3 (vs. RLS 1) was an independent risk factor for fewer days alive and out of hospital (p ≤ 0.008) and longer post-operative hospital stay (p ≤ 0.02) for all 5 operations, and for all secondary outcomes after coarctation or interrupted arch with VSD repair and Norwood (p ≤ 0.03). Outcomes for RLS 1 versus 2 did not differ consistently. RLS alone explained 5% (tetralogy of Fallot repair) to 20% (Norwood) of variation in the primary outcome.
Conclusions: Adjusting for pre-operative factors, residual lesions after congenital cardiac surgery impacted in-hospital outcomes across operative complexity with greatest impact following complex operations. Minor residual lesions had minimal impact. These findings may provide guidance for surgeons when considering short-term risks and benefits of returning to bypass to repair residual lesions.
Keywords: Residual Lesion Score; days alive and out of the hospital; outcomes.
Copyright © 2021 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by grants (U24HL135691, U10HL068270, HL109818, HL109778, HL109816, HL109743, HL109741, HL109673, HL068270, HL109781, HL135665, HL135680) from the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH). Drs. Nathan and Anderson were supported by K23 grants (NHLBI/NIH HL119600and HL133454, respectively). The views expressed in this paper are those of the authors and do not necessarily represent the views of the NHLBI, NIH, or U.S. Department of Health and Human Services. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
One Step Closer to Understanding What Is Good Enough.J Am Coll Cardiol. 2021 May 18;77(19):2395-2397. doi: 10.1016/j.jacc.2021.03.302. J Am Coll Cardiol. 2021. PMID: 33985684 No abstract available.
References
-
- Connor JA, Gauvreau K, Jenkins KJ. Factors associated with increased resource utilization for congenital heart disease. Pediatrics 2005;116(3);689–695. - PubMed
-
- Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, Iezzoni LI. Consensus based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg 2002; 123(1):110–118. - PubMed
-
- Jenkin KJ. Risk adjustment for congenital heart surgery: The RACHS-1 method Seminars in Thorac and Cardiovasc Surg: Pediatric Cardiac Surgery Annual. 2004; 7(1):180–184. - PubMed
-
- Connor JA and Jenkins KJ. Factors associated with increased resource utilization for congenital heart disease. In: Congenital Heart Defects: From Origin to Treatment. Editors Wyszynski D and Correa A. Oxford University, New York, 2010.
-
- Nathan M, Karamichalis J. Quality Improvement: Surgical Performance. Technical Performance Score as a performance measure for congenital heart surgery. In Sellke/Sabiston and Spencer’s Surgery of the Chest, 9th edition, 2015; Chapter 134.
Publication types
MeSH terms
Grants and funding
- UG1 HL135665/HL/NHLBI NIH HHS/United States
- UG1 HL135666/HL/NHLBI NIH HHS/United States
- U10 HL109818/HL/NHLBI NIH HHS/United States
- U10 HL109741/HL/NHLBI NIH HHS/United States
- UG1 HL135680/HL/NHLBI NIH HHS/United States
- U10 HL109781/HL/NHLBI NIH HHS/United States
- U24 HL135691/HL/NHLBI NIH HHS/United States
- U10 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- U10 HL109778/HL/NHLBI NIH HHS/United States
- K23 HL133454/HL/NHLBI NIH HHS/United States
- UG1 HL135646/HL/NHLBI NIH HHS/United States
- UG1 HL135685/HL/NHLBI NIH HHS/United States
- U10 HL109816/HL/NHLBI NIH HHS/United States
- UG1 HL135689/HL/NHLBI NIH HHS/United States
- U10 HL109743/HL/NHLBI NIH HHS/United States
- U10 HL109673/HL/NHLBI NIH HHS/United States
- K23 HL119600/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
