

Patterns of Clinical Progression in Radiorecurrent High-risk Prostate Cancer
- PMID: 33985797
- PMCID: PMC10262978
- DOI: 10.1016/j.eururo.2021.04.035
Patterns of Clinical Progression in Radiorecurrent High-risk Prostate Cancer
Abstract
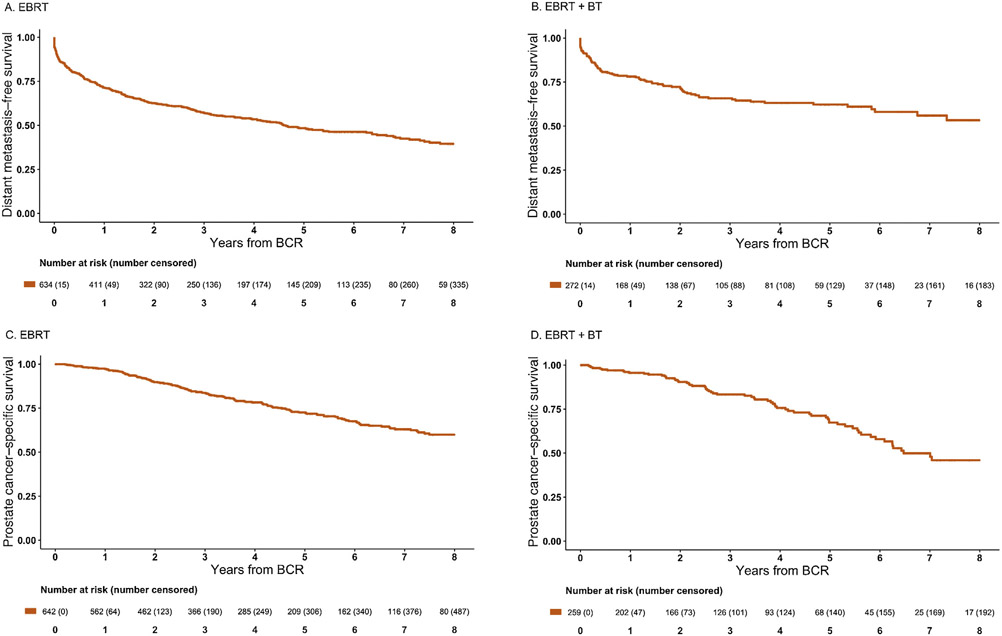
The natural history of radiorecurrent high-risk prostate cancer (HRPCa) is not well-described. To better understand its clinical course, we evaluated rates of distant metastases (DM) and prostate cancer-specific mortality (PCSM) in a cohort of 978 men with radiorecurrent HRPCa who previously received either external beam radiation therapy (EBRT, n = 654, 67%) or EBRT + brachytherapy (EBRT + BT, n = 324, 33%) across 15 institutions from 1997 to 2015. In men who did not die, median follow-up after treatment was 8.9 yr and median follow-up after biochemical recurrence (BCR) was 3.7 yr. Local and systemic therapy salvage, respectively, were delivered to 21 and 390 men after EBRT, and eight and 103 men after EBRT + BT. Overall, 435 men developed DM, and 248 were detected within 1 yr of BCR. Measured from time of recurrence, 5-yr DM rates were 50% and 34% after EBRT and EBRT + BT, respectively. Measured from BCR, 5-yr PCSM rates were 27% and 29%, respectively. Interval to BCR was independently associated with DM (p < 0.001) and PCSM (p < 0.001). These data suggest that radiorecurrent HRPCa has an aggressive natural history and that DM is clinically evident early after BCR. These findings underscore the importance of further investigations into upfront risk assessment and prompt systemic evaluation upon recurrence in HRPCa. PATIENT SUMMARY: High-risk prostate cancer that recurs after radiation therapy is an aggressive disease entity and spreads to other parts of the body (metastases). Some 60% of metastases occur within 1 yr. Approximately 30% of these patients die from their prostate cancer.
Keywords: Biochemical recurrence; Brachytherapy boost; EBRT; External beam radiation therapy; High-risk prostate cancer; Prostate cancer; Radiorecurrence; Recurrent prostate cancer.
Copyright © 2021 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
High-risk Prostate Cancer Treated with Radiation Therapy: Opportunities to Reduce Cancer Mortality after Biochemical Failure.Eur Urol. 2021 Aug;80(2):147-148. doi: 10.1016/j.eururo.2021.05.023. Epub 2021 May 28. Eur Urol. 2021. PMID: 34053781 No abstract available.
References
-
- Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006;65:965–74. - PubMed
-
- Spratt DE, McHugh DJ, Morris MJ, Morgans AK. Management of biochemically recurrent prostate cancer: ensuring the right treatment of the right patient at the right time. Am Soc Clin Oncol Educ Book 2018;38:355–62. - PubMed
-
- Ost P, Reynders D, Decaestecker K, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase II trial. J Clin Oncol 2017;36:446–53. - PubMed
-
- Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994;81:515–26.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
