

Reducing antibiotic treatment duration for ventilator-associated pneumonia (REGARD-VAP): a trial protocol for a randomised clinical trial
- PMID: 33986070
- PMCID: PMC8126270
- DOI: 10.1136/bmjopen-2021-050105
Reducing antibiotic treatment duration for ventilator-associated pneumonia (REGARD-VAP): a trial protocol for a randomised clinical trial
Abstract
Introduction: Ventilator-associated pneumonia (VAP) is the most common nosocomial infection in intensive care units (ICUs). Using short-course antibiotics to treat VAP caused by Gram-negative non-fermenting bacteria has been reported to be associated with excess pneumonia recurrences. The "REducinG Antibiotic tReatment Duration for Ventilator-Associated Pneumonia" (REGARD-VAP) trial aims to provide evidence for using a set of reproducible clinical criteria to shorten antibiotic duration for individualised treatment duration of VAP.
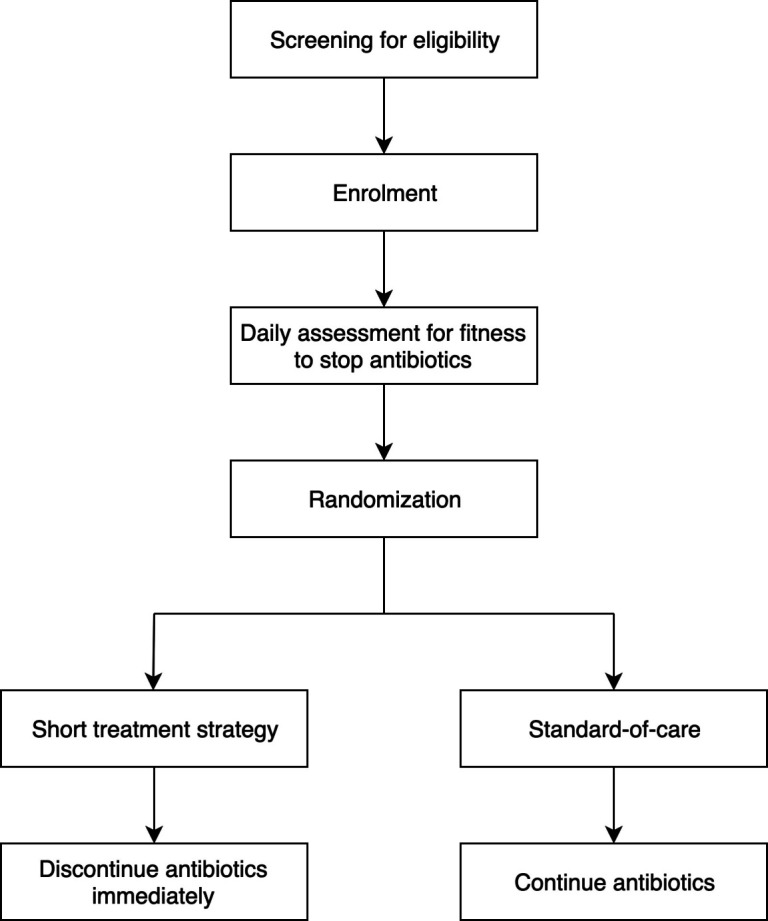
Methods and analysis: This is a randomised controlled hierarchical non-inferiority-superiority trial being conducted in ICUs across Nepal, Thailand and Singapore. The primary outcome is a composite endpoint of death and pneumonia recurrence at day 60. Secondary outcomes include ventilator-associated events, multidrug-resistant organism infection or colonisation, total duration of antibiotic exposure, mechanical ventilation and hospitalisation. Adult patients who satisfy the US Centers for Disease Control and Prevention National Healthcare Safety Network VAP diagnostic criteria are enrolled. Participants are assessed daily until fever subsides for >48 hours and have stable blood pressure, then randomised to a short duration treatment strategy or a standard-of-care duration arm. Antibiotics may be stopped as early as day 3 if respiratory cultures are negative, and day 5 if respiratory cultures are positive in the short-course arm. Participants receiving standard-of-care will receive antibiotics for at least 8 days. Study participants are followed for 60 days after enrolment. An estimated 460 patients will be required to achieve 80% power to determine non-inferiority with a margin of 12%. All outcomes are compared by absolute risk differences. The conclusion of non-inferiority, and subsequently superiority, will be based on unadjusted and adjusted analyses in both the intention-to-treat and per-protocol populations.
Ethics and dissemination: The study has received approvals from the Oxford Tropical Research Ethics Committee and the respective study sites. Results will be disseminated to patients, their caregivers, physicians, the funders, the critical care societies and other researchers.
Trial registration number: NCT03382548.
Keywords: infectious diseases; intensive & critical care; statistics & research methods.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Kalil AC, Metersky ML, Klompas M, et al. . Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases Society of America and the American thoracic Society. Clin Infect Dis [Internet] 2016;63:e61–111. 10.1093/cid/ciw353 - DOI - PMC - PubMed
-
- Stebbings AE, Ti TY, Tan WC. Hospital acquired pneumonia in the medical intensive care unit--a prospective study. Singapore Med J 1999;40:508–12. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical