

Fugitive aerosols in the intensive care unit: a narrative review
- PMID: 33987290
- PMCID: PMC8105852
- DOI: 10.21037/atm-20-2280
Fugitive aerosols in the intensive care unit: a narrative review
Abstract
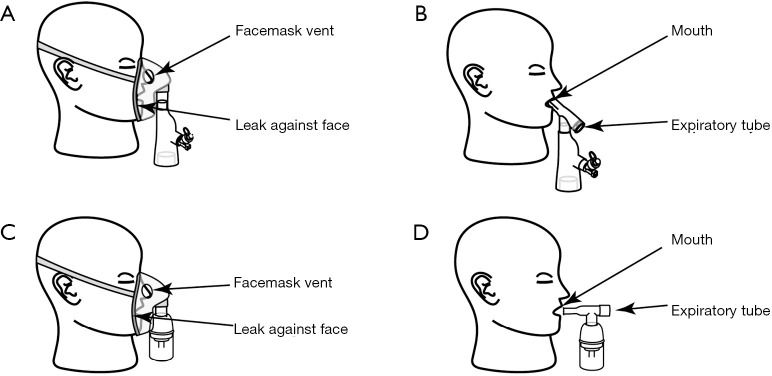
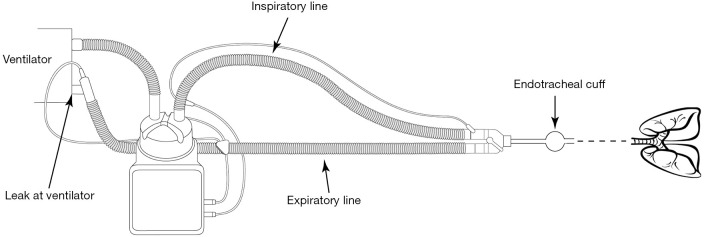
The risk of unintended inhalation of fugitive aerosols is becoming a topic of increasing interest in the healthcare arena. These fugitive aerosols may be bioaerosols, generated by the patient themselves through cough or sneeze, or they may be therapeutic medical aerosols, generated by therapeutic medical aerosol generators with the intent of delivery to a specific patient's respiratory tract. This review focus' on therapeutic aerosols in the intensive care unit (ICU) only, those typically generated by nebulisers. In the intensive care environment, patients are generally in receipt of ventilatory support, and the literature suggests that these different support interventions influence fugitive therapeutic medical aerosol emissions in a variety of ways. Predominant ventilatory support interventions include, but are not limited to, invasive mechanical ventilation (MV), non-invasive mechanical ventilation (NIV), high flow nasal therapy (HFNT), and supplemental oxygen delivery in spontaneously breathing patients. Further, factors such as nebuliser type, patient interface, patient breathing pattern, nebuliser position in the patient breathing circuit and medication formulation characteristics also have been shown to exert influence on aerosol concentrations and distance from the source. Here we present the state of the art knowledge in this, as yet, poorly described field of research, and identify the key risks, and subsequently, opportunities to mitigate the risks of unintended exposure of both patients and bystanders during and for periods following the administration of therapeutic aerosols.
Keywords: Aerosols; exposure; fugitive; intensive care unit (ICU); jet nebulizer (JN); secondary inhalation; vibrating mesh nebuliser (VMN).
2021 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm-20-2280). The series “Medical Aerosol in Acute and Critical Care” was commissioned by the editorial office without any funding or sponsorship. CO, JAM, and MAB reports grants from Irish Research Council, during the conduct of the study. MJ, AO, and RM reports personal fees from Aerogen Limited, outside the submitted work. The authors have no other conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources