

Association of Post-discharge Service Types and Timing with 30-Day Readmissions, Length of Stay, and Costs
- PMID: 33987792
- PMCID: PMC8342719
- DOI: 10.1007/s11606-021-06708-6
Association of Post-discharge Service Types and Timing with 30-Day Readmissions, Length of Stay, and Costs
Abstract
Background: Although early follow-up after discharge from an index admission (IA) has been postulated to reduce 30-day readmission, some researchers have questioned its efficacy, which may depend upon the likelihood of readmission at a given time and the health conditions contributing to readmissions.
Objective: To investigate the relationship between post-discharge services utilization of different types and at different timepoints and unplanned 30-day readmission, length of stay (LOS), and inpatient costs.
Design, setting, and participants: The study sample included 583,199 all-cause IAs among 2014 Medicare fee-for-service beneficiaries that met IA inclusion criteria.
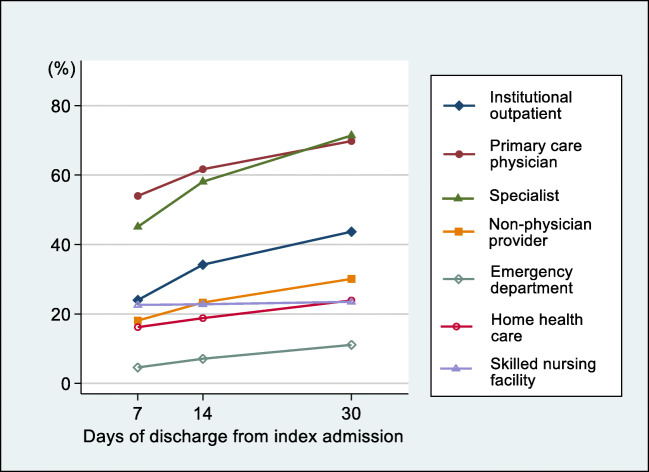
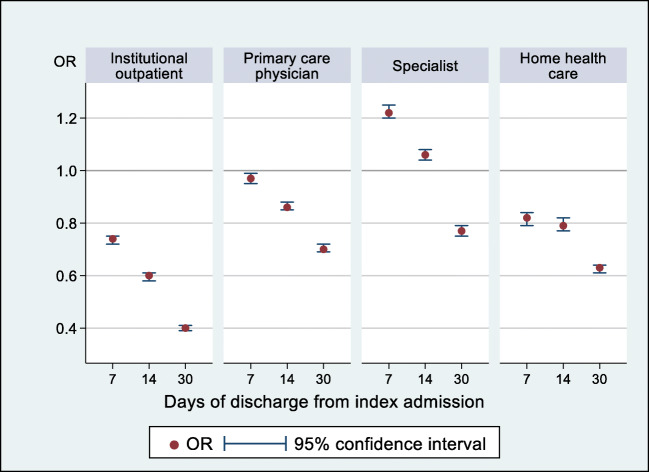
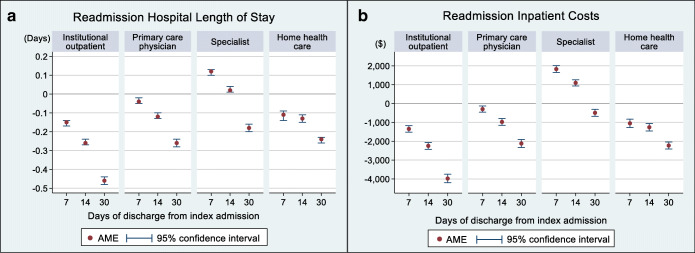
Main measures: The outcomes were probability of 30-day readmission, average readmission LOS per IA discharge, and average readmission inpatient cost per IA discharge. The primary independent variables were 7 post-discharge health services (institutional outpatient, primary care physician, specialist, non-physician provider, emergency department (ED), home health care, skilled nursing facility) utilized within 7 days, 14 days, and 30 days of IA discharge. To examine the association with post-discharge services utilization, we employed multivariable logistic regressions for 30-day readmissions and two-part models for LOS and inpatient costs.
Key results: Among all IA discharges, the probability of unplanned 30-day readmission was 0.1176, the average readmission LOS per discharge was 0.67 days, and the average inpatient cost per discharge was $5648. Institutional outpatient, home health care, and primary care physician visits at all timepoints were associated with decreased readmission and resource utilization. Conversely, 7-day and 14-day specialist visits were positively associated with all three outcomes, while 30-day visits were negatively associated. ED visits were strongly associated with increases in all three outcomes at all timepoints.
Conclusion: Post-discharge services of different types and at different timepoints have varying impacts on 30-day readmission, LOS, and costs. These impacts should be considered when coordinating post-discharge follow-up, and their drivers should be further explored to reduce readmission throughout the health care system.
Keywords: Hospital Readmission Reduction Program; all-cause index admission; post-discharge services utilization; service types; unplanned 30-day readmission.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- McAlister FA, Youngson E, Kaul P, Ezekowitz JA. Early follow-up after a heart failure exacerbation. Circ Heart Fail. 2016;9(9). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
