

Mechanistic insights into cell-free hemoglobin-induced injury during septic shock
- PMID: 33989079
- PMCID: PMC8289364
- DOI: 10.1152/ajpheart.00092.2021
Mechanistic insights into cell-free hemoglobin-induced injury during septic shock
Abstract
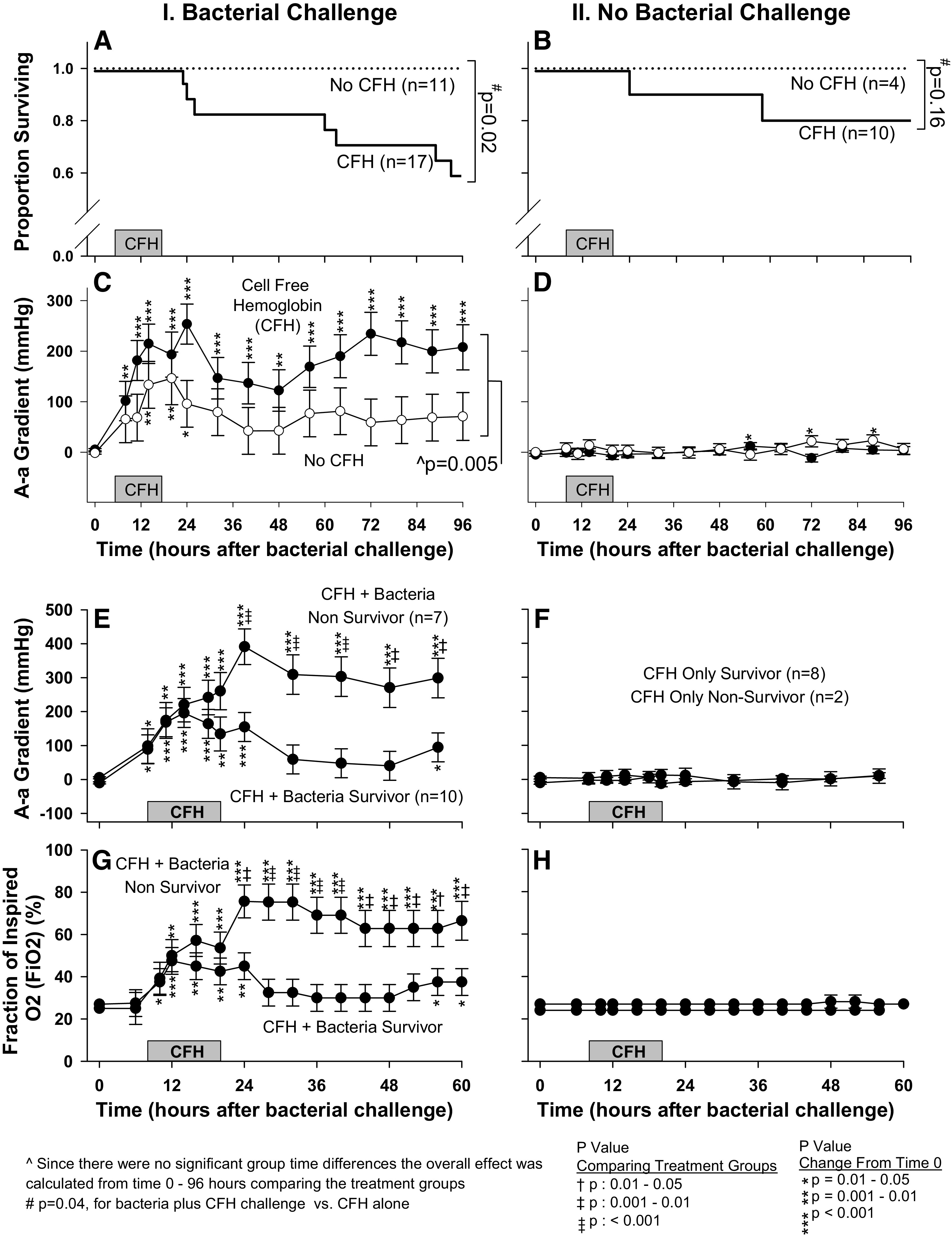
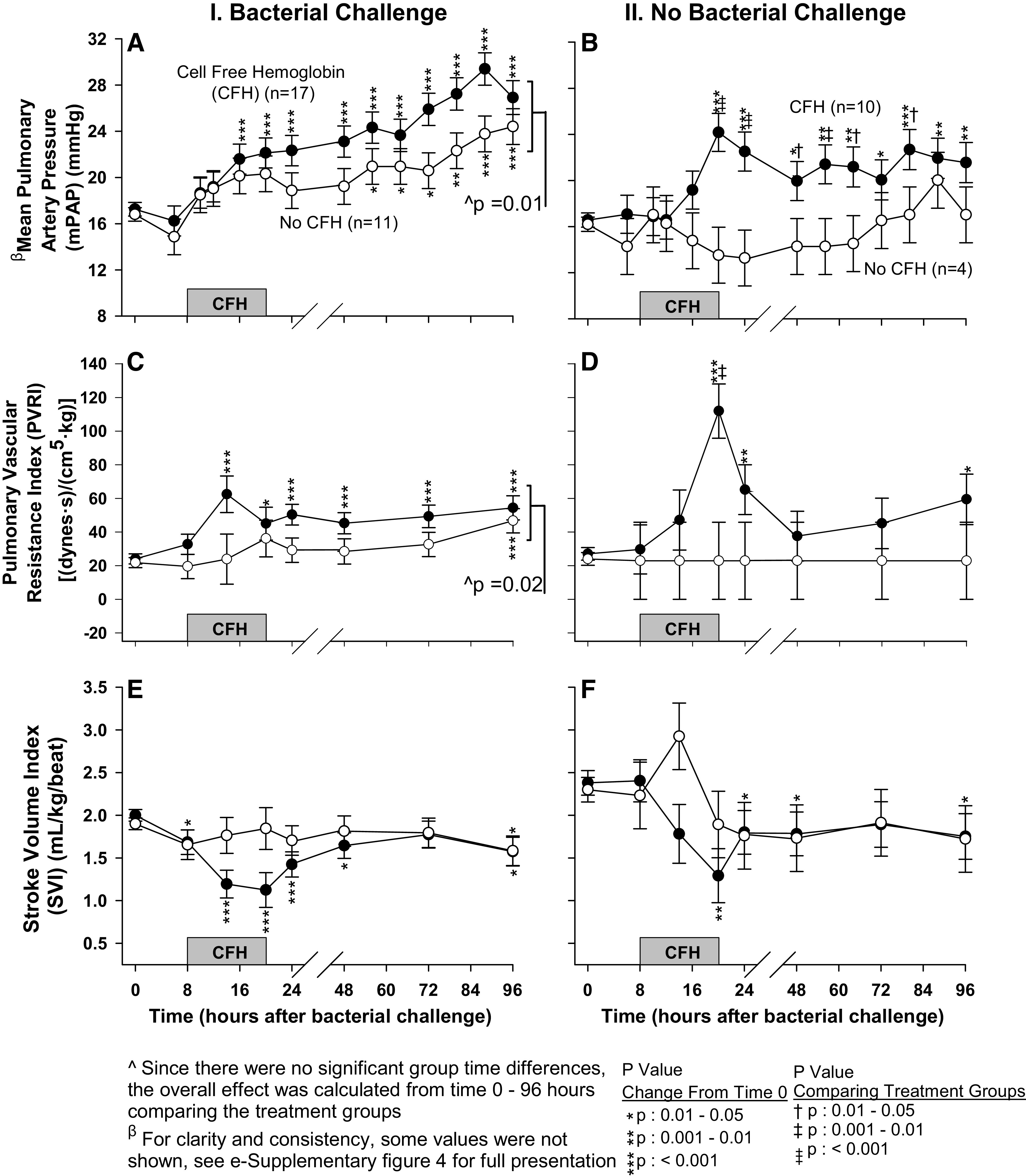
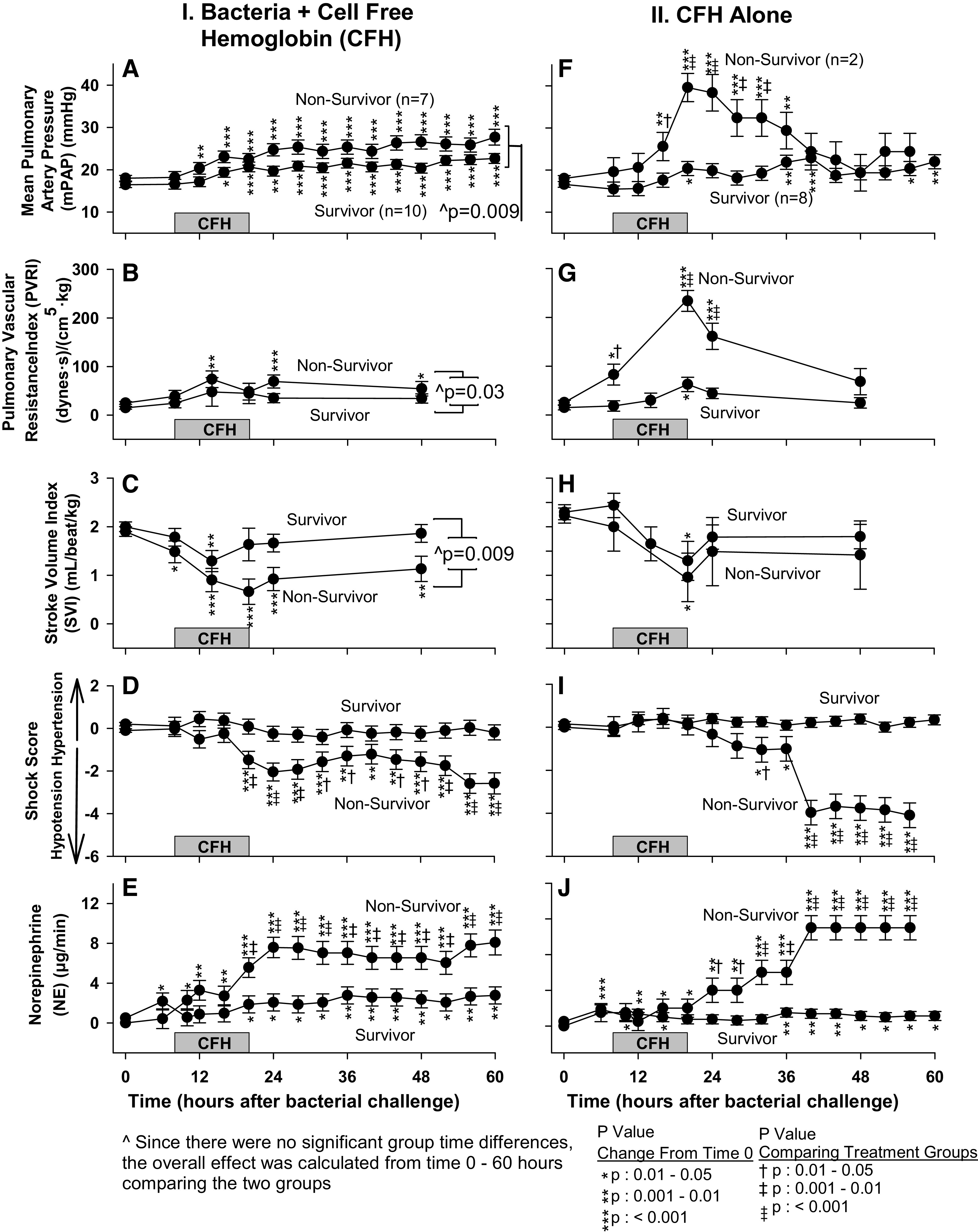
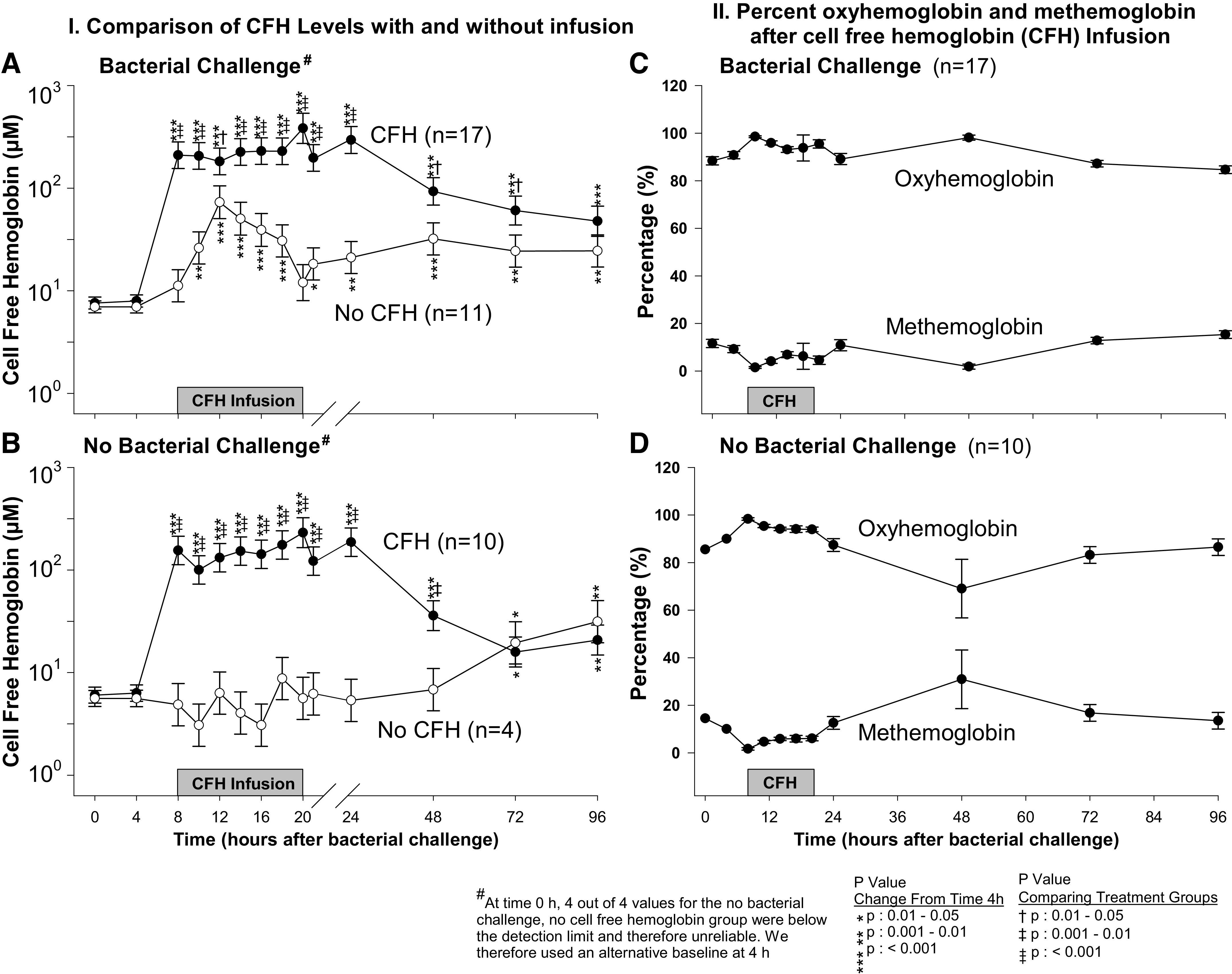
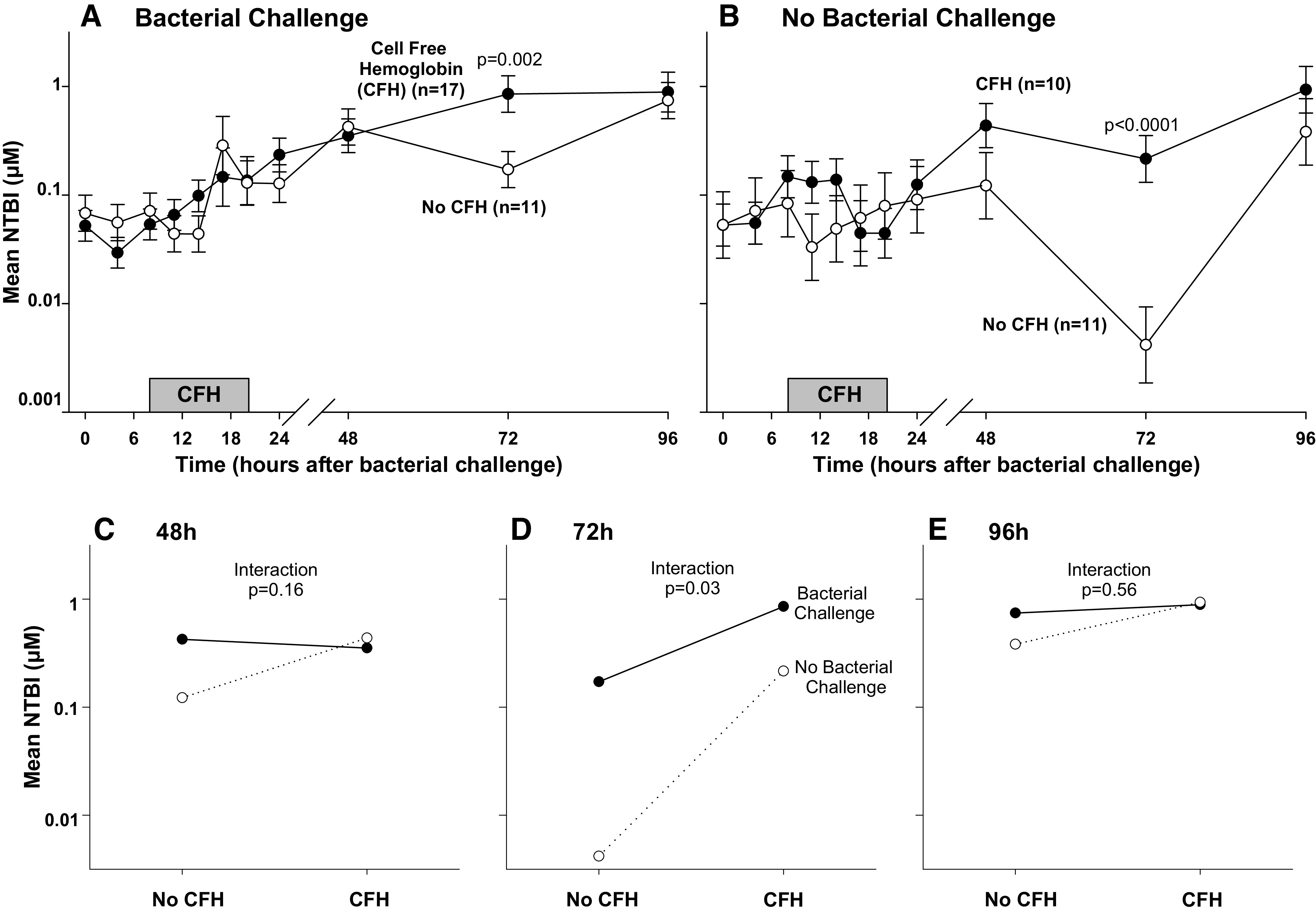
Cell-free hemoglobin (CFH) levels are elevated in septic shock and are higher in nonsurvivors. Whether CFH is only a marker of sepsis severity or is involved in pathogenesis is unknown. This study aimed to investigate whether CFH worsens sepsis-associated injuries and to determine potential mechanisms of harm. Fifty-one, 10-12 kg purpose-bred beagles were randomized to receive Staphylococcus aureus intrapulmonary challenges or saline followed by CFH infusions (oxyhemoglobin >80%) or placebo. Animals received antibiotics and intensive care support for 96 h. CFH significantly increased mean pulmonary arterial pressures and right ventricular afterload in both septic and nonseptic animals, effects that were significantly greater in nonsurvivors. These findings are consistent with CFH-associated nitric oxide (NO) scavenging and were associated with significantly depressed cardiac function, and worsened shock, lactate levels, metabolic acidosis, and multiorgan failure. In septic animals only, CFH administration significantly increased mean alveolar-arterial oxygenation gradients, also to a significantly greater degree in nonsurvivors. CFH-associated iron levels were significantly suppressed in infected animals, suggesting that bacterial iron uptake worsened pneumonia. Notably, cytokine levels were similar in survivors and nonsurvivors and were not predictive of outcome. In the absence and presence of infection, CFH infusions resulted in pulmonary hypertension, cardiogenic shock, and multiorgan failure, likely through NO scavenging. In the presence of infection alone, CFH infusions worsened oxygen exchange and lung injury, presumably by supplying iron that promoted bacterial growth. CFH elevation, a known consequence of clinical septic shock, adversely impacts sepsis outcomes through more than one mechanism, and is a biologically plausible, nonantibiotic, noncytokine target for therapeutic intervention.NEW & NOTEWORTHY Cell-free hemoglobin (CFH) elevations are a known consequence of clinical sepsis. Using a two-by-two factorial design and extensive physiological and biochemical evidence, we found a direct mechanism of injury related to nitric oxide scavenging leading to pulmonary hypertension increasing right heart afterload, depressed cardiac function, worsening circulatory failure, and death, as well as an indirect mechanism related to iron toxicity. These discoveries alter conventional thinking about septic shock pathogenesis and provide novel therapeutic approaches.
Keywords: cell-free hemoglobin; iron; septic shock.
Conflict of interest statement
M.T.G. and D.B.K-S. are coinventors in patents for the treatment of hemolysis (Patent No. 8980871 and 9114109). M.T.G. and J.T. are coinventors of pending patent applications and planned patents directed to the use of recombinant neuroglobin and heme-based molecules as antidotes for CO poisoning, which have recently been licensed by Globin Solutions Inc. M.T.G. and J.T. are shareholders and directors in Globin Solutions Inc. In addition, and unrelated to CO poisoning, M.T.G. and D.B.K-S. are coinventors on patents directed to the use of nitrite salts in cardiovascular diseases, which have been licensed by the United Therapeutics and Hope Pharmaceuticals, and M.T.G. is a coinvestigator in a research collaboration with Bayer Pharmaceuticals to evaluate riociguat as a treatment for patients with sudden cardiac death.
Figures

Comment in
-
Enemies at the gate: how cell-free hemoglobin and bacterial infection can cooperate to drive acute lung injury during sepsis.Am J Physiol Heart Circ Physiol. 2021 Jul 1;321(1):H131-H134. doi: 10.1152/ajpheart.00283.2021. Epub 2021 Jun 4. Am J Physiol Heart Circ Physiol. 2021. PMID: 34085840 No abstract available.
References
-
- Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, Kadri SS, Angus DC, Danner RL, Fiore AE, Jernigan JA, Martin GS, Septimus E, Warren DK, Karcz A, Chan C, Menchaca JT, Wang R, Gruber S, Klompas M; CDC Prevention Epicenter Program. Incidence and trends of sepsis in US Hospitals using clinical vs claims data, 2009-2014. JAMA 318: 1241–1249, 2017. doi:10.1001/jama.2017.13836. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous