

Effects of nurse-to-patient ratio legislation on nurse staffing and patient mortality, readmissions, and length of stay: a prospective study in a panel of hospitals
- PMID: 33989553
- PMCID: PMC8408834
- DOI: 10.1016/S0140-6736(21)00768-6
Effects of nurse-to-patient ratio legislation on nurse staffing and patient mortality, readmissions, and length of stay: a prospective study in a panel of hospitals
Abstract
Background: Substantial evidence indicates that patient outcomes are more favourable in hospitals with better nurse staffing. One policy designed to achieve better staffing is minimum nurse-to-patient ratio mandates, but such policies have rarely been implemented or evaluated. In 2016, Queensland (Australia) implemented minimum nurse-to-patient ratios in selected hospitals. We aimed to assess the effects of this policy on staffing levels and patient outcomes and whether both were associated.
Methods: For this prospective panel study, we compared Queensland hospitals subject to the ratio policy (27 intervention hospitals) and those that discharged similar patients but were not subject to ratios (28 comparison hospitals) at two timepoints: before implementation of ratios (baseline) and 2 years after implementation (post-implementation). We used standardised Queensland Hospital Admitted Patient Data, linked with death records, to obtain data on patient characteristics and outcomes (30-day mortality, 7-day readmissions, and length of stay [LOS]) for medical-surgical patients and survey data from 17 010 medical-surgical nurses in the study hospitals before and after policy implementation. Survey data from nurses were used to measure nurse staffing and, after linking with standardised patient data, to estimate the differential change in outcomes between patients in intervention and comparison hospitals, and determine whether nurse staffing changes were related to it.
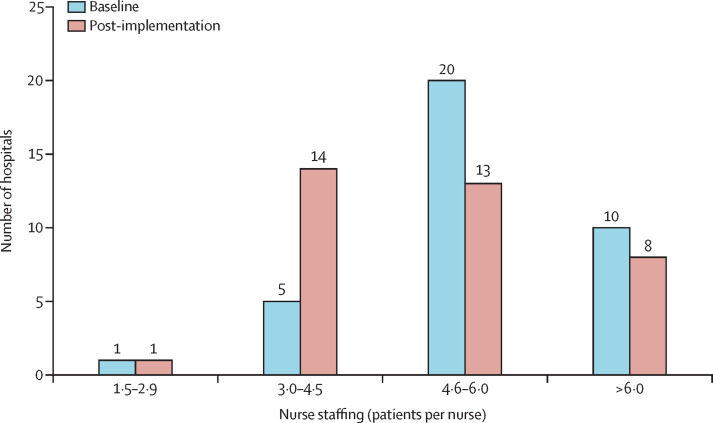
Findings: We included 231 902 patients (142 986 in intervention hospitals and 88 916 in comparison hospitals) assessed at baseline (2016) and 257 253 patients (160 167 in intervention hospitals and 97 086 in comparison hospitals) assessed in the post-implementation period (2018). After implementation, mortality rates were not significantly higher than at baseline in comparison hospitals (adjusted odds ratio [OR] 1·07, 95% CI 0·97-1·17, p=0·18), but were significantly lower than at baseline in intervention hospitals (0·89, 0·84-0·95, p=0·0003). From baseline to post-implementation, readmissions increased in comparison hospitals (1·06, 1·01-1·12, p=0·015), but not in intervention hospitals (1·00, 0·95-1·04, p=0·92). Although LOS decreased in both groups post-implementation, the reduction was more pronounced in intervention hospitals than in comparison hospitals (adjusted incident rate ratio [IRR] 0·95, 95% CI 0·92-0·99, p=0·010). Staffing changed in hospitals from baseline to post-implementation: of the 36 hospitals with reliable staffing measures, 30 (83%) had more than 4·5 patients per nurse at baseline, with the number decreasing to 21 (58%) post-implementation. The majority of change was at intervention hospitals, and staffing improvements by one patient per nurse produced reductions in mortality (OR 0·93, 95% CI 0·86-0·99, p=0·045), readmissions (0·93, 0·89-0·97, p<0·0001), and LOS (IRR 0·97, 0·94-0·99, p=0·035). In addition to producing better outcomes, the costs avoided due to fewer readmissions and shorter LOS were more than twice the cost of the additional nurse staffing.
Interpretation: Minimum nurse-to-patient ratio policies are a feasible approach to improve nurse staffing and patient outcomes with good return on investment.
Funding: Queensland Health, National Institutes of Health, National Institute of Nursing Research.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Patient safety: the value of the nurse.Lancet. 2021 May 22;397(10288):1861-1863. doi: 10.1016/S0140-6736(21)00981-8. Epub 2021 May 11. Lancet. 2021. PMID: 33989554 No abstract available.
-
Minimum nurse-to-patient Ratios Improve Staffing, Patient Outcomes.Am J Nurs. 2021 Sep 1;121(9):57. doi: 10.1097/01.NAJ.0000790644.96356.96. Am J Nurs. 2021. PMID: 34438432
-
From nurse-to-patient ratio to optimal team composition.Lancet. 2021 Sep 25;398(10306):1129-1130. doi: 10.1016/S0140-6736(21)01818-3. Lancet. 2021. PMID: 34563288 No abstract available.
-
Mandated nursing ratios decrease mortality and costs in the hospital, and what about the ICU?Anaesth Crit Care Pain Med. 2021 Dec;40(6):100977. doi: 10.1016/j.accpm.2021.100977. Epub 2021 Nov 5. Anaesth Crit Care Pain Med. 2021. PMID: 34748941 No abstract available.
References
-
- WHO 2020—Year of the Nurse and the Midwife. 2021. https://www.who.int/campaigns/annual-theme/year-of-the-nurse-and-the-mid...
-
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288:1987–1993. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
