

Kidney Transplant List Status and Outcomes in the ISCHEMIA-CKD Trial
- PMID: 33989711
- PMCID: PMC8319110
- DOI: 10.1016/j.jacc.2021.05.001
Kidney Transplant List Status and Outcomes in the ISCHEMIA-CKD Trial
Abstract
Background: Patients with chronic kidney disease (CKD) and coronary artery disease frequently undergo preemptive revascularization before kidney transplant listing.
Objectives: In this post hoc analysis from ISCHEMIA-CKD (International Study of Comparative Health Effectiveness of Medical and Invasive Approaches-Chronic Kidney Disease), we compared outcomes of patients not listed versus those listed according to management strategy.
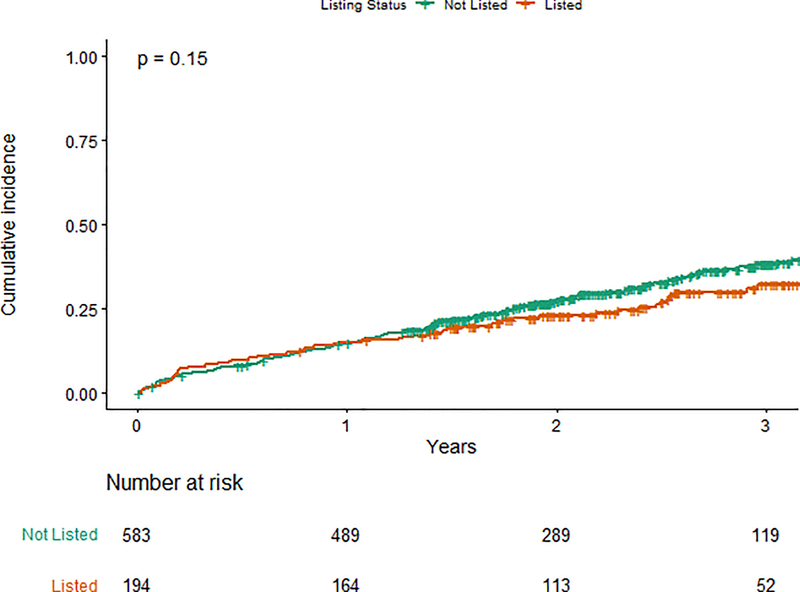
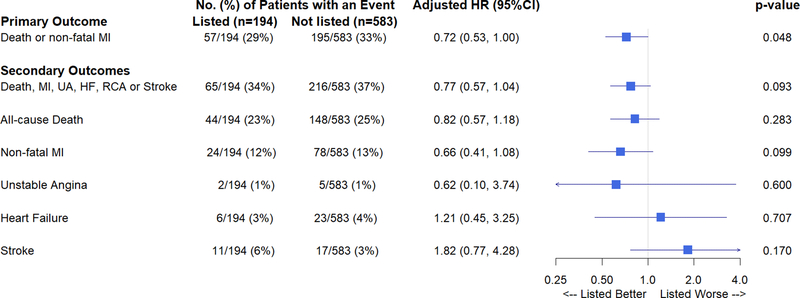
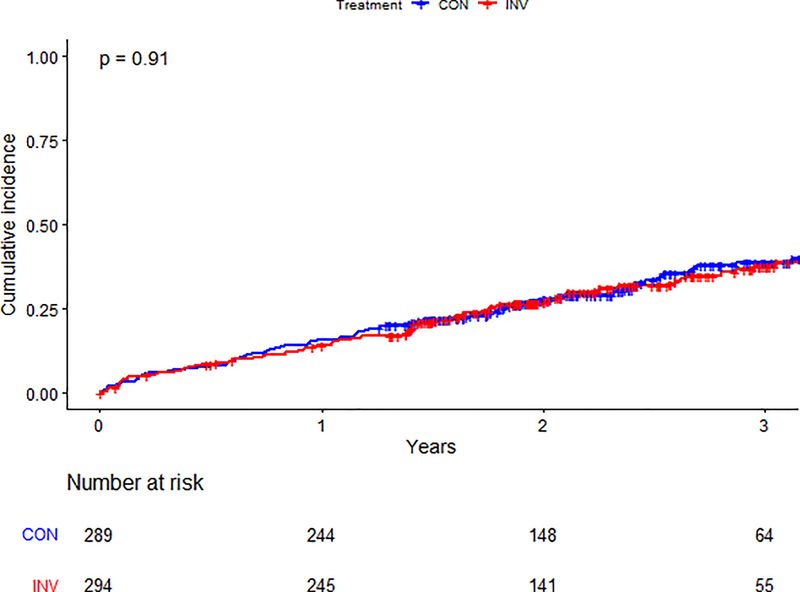
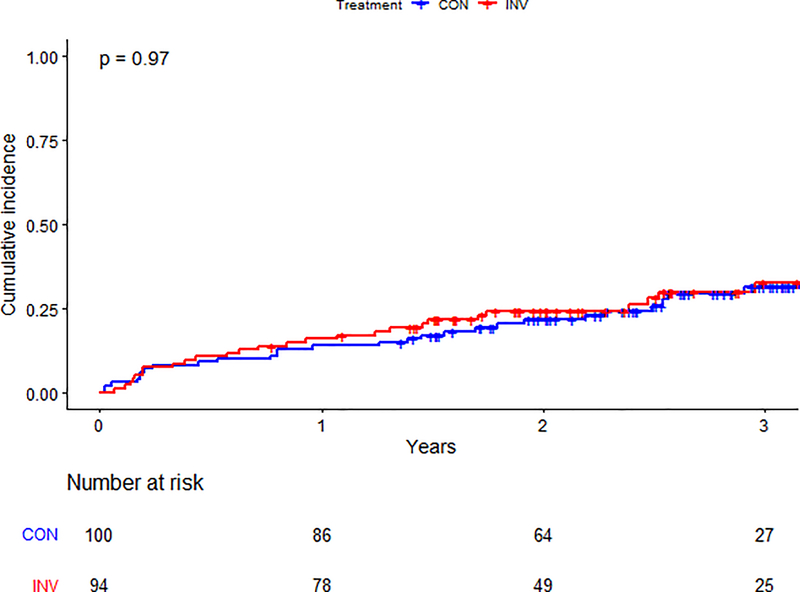
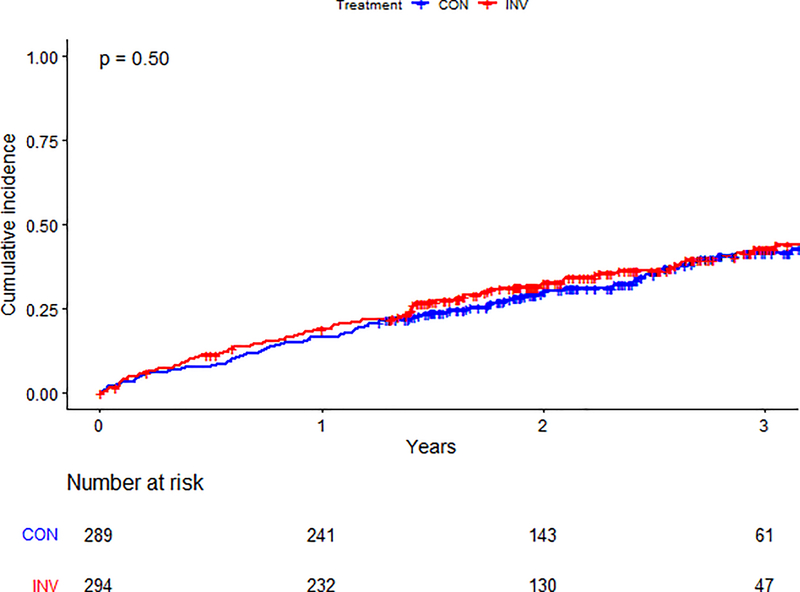
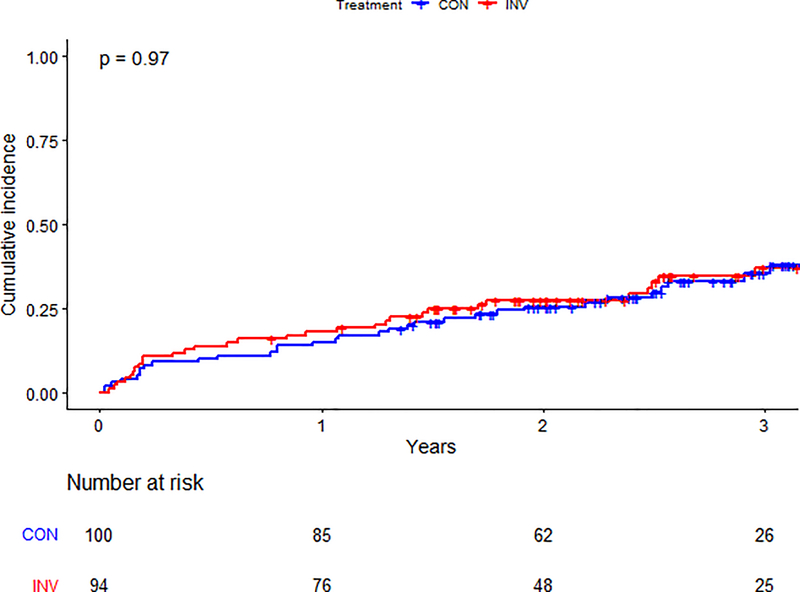
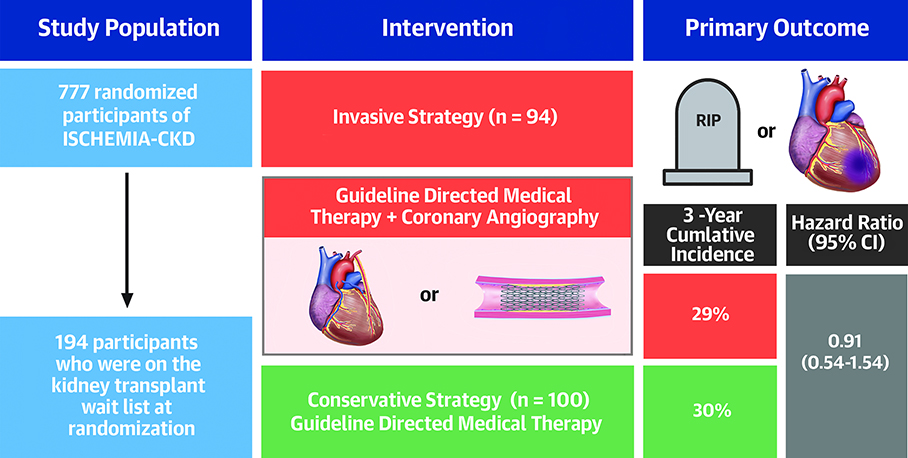
Methods: In the ISCHEMIA-CKD trial (n = 777), 194 patients (25%) with chronic coronary syndromes and at least moderate ischemia were listed for transplant. The primary (all-cause mortality or nonfatal myocardial infarction) and secondary (death, nonfatal myocardial infarction, hospitalization for unstable angina, heart failure, resuscitated cardiac arrest, or stroke) outcomes were analyzed using Cox multivariable modeling. Heterogeneity of randomized treatment effect between listed versus not listed groups was assessed.
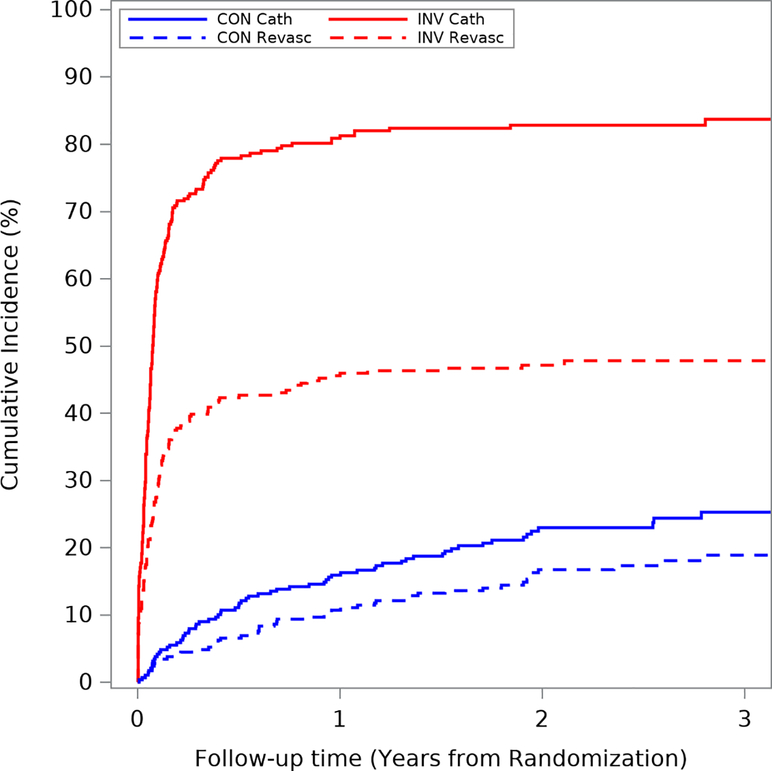
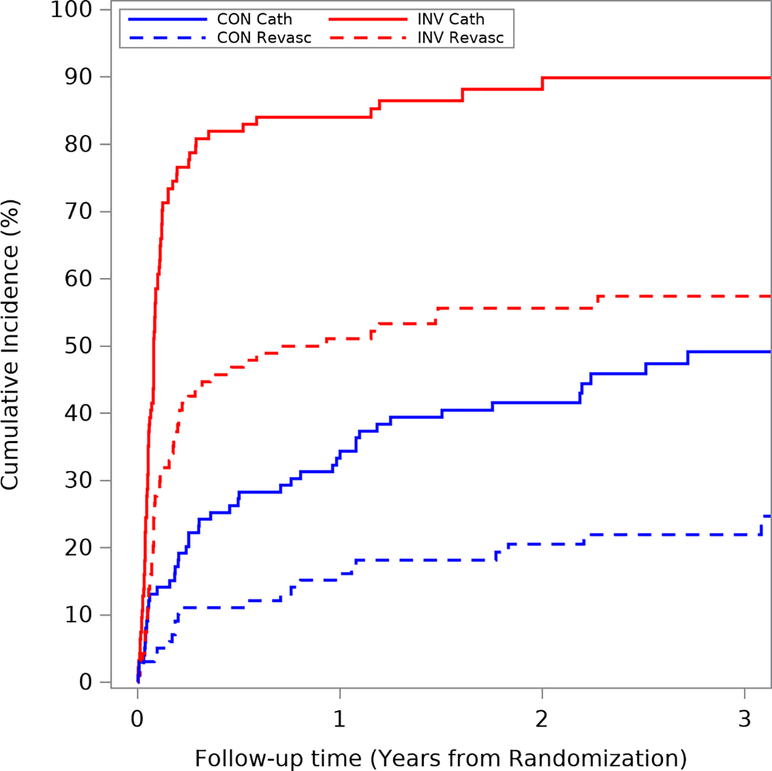
Results: Compared with those not listed, listed patients were younger (60 years vs 65 years), were less likely to be of Asian race (15% vs 29%), were more likely to be on dialysis (83% vs 44%), had fewer anginal symptoms, and were more likely to have coronary angiography and coronary revascularization irrespective of treatment assignment. Among patients assigned to an invasive strategy versus conservative strategy, the adjusted hazard ratios for the primary outcome were 0.91 (95% confidence interval [CI]: 0.54-1.54) and 1.03 (95% CI: 0.78-1.37) for those listed and not listed, respectively (pinteraction= 0.68). Adjusted hazard ratios for secondary outcomes were 0.89 (95% CI: 0.55-1.46) in listed and 1.17 (95% CI: 0.89-1.53) in those not listed (pinteraction = 0.35).
Conclusions: In ISCHEMIA-CKD, an invasive strategy in kidney transplant candidates did not improve outcomes compared with conservative management. These data do not support routine coronary angiography or revascularization in patients with advanced CKD and chronic coronary syndromes listed for transplant. (ISCHEMIA-Chronic Kidney Disease Trial [ISCHEMIA-CKD]; NCT01985360).
Keywords: chronic kidney disease; coronary angiography; coronary revascularization; ischemic heart disease; kidney transplantation; medical therapy.
Copyright © 2021 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was funded by the National Institutes of Health (NIH) (grants U01HL117904 and U01HL117905). This project was supported by grants from Arbor Pharmaceuticals and AstraZeneca Pharmaceuticals. Devices or medications were provided by Abbott Vascular (previously St. Jude Medical), Medtronic, Phillips (previously Volcano Corporation), and Omron Healthcare. Medications provided by Arbor Pharmaceuticals, AstraZeneca Pharmaceuticals, Espero Pharmaceuticals, Merck Sharp & Dohme Corp., and Sunivion Pharmaceuticals. The contents are solely the responsibility of the authors and do not necessarily represent official views of the National Heart, Lung, and Blood Institute, the National Institutes of Health, or the Department of Health and Human Services. Dr Herzog has received personal fees from the National Heart, Lung, and Blood Institute (NHLBI)/NIH during the conduct of the study; has received research grants from Amgen, Relypsa, Bristol Myers Squibb, National Institute of Diabetes and Digestive and Kidney Diseases/NIH, University of British Columbia; and has received other support from Abbvie, Amgen, AstraZeneca, Corvidia, Diamedica, FibroGen, Janssen, NxStage, Pfizer, Relypsa, Sanifit, University of Oxford, Bristol Myers Squibb, UpToDate, Boston Scientific, General Electric, Johnson & Johnson, Merck, and Hennepin Healthcare. Drs. Simegn, Costa, Mathew, El-Hajjar, Gulati, Maldonao, Madero, Anthopolos, Maron, and Mr. Xu has received research grants from the National Heart, Lung, and Blood Institute during the conduct of the study. Dr Daugas has received personal fees from Amgen, GlaxoSmithKline, and AstraZeneca; has received grants from Agence Nationale pour la Recherche/ Direction Générale de l'Offre de Soins; and has received nonfinancial support from Amgen. Dr Fleg was an employee of the NHLBI during the conduct of the study. Dr Stone has received speaker or other honoraria from Cook and Terumo; has served as a consultant to Valfix, TherOx, Vascular Dynamics, Robocath, HeartFlow, Gore, Ablative Solutions, Miracor, Neovasc, V-Wave, Abiomed, Ancora, MAIA Pharmaceuticals, Vectorious, Reva, Matrizyme, Cardiomech, Elucid Bio, and Occlutech; and has equity/options from Ancora, Cagent, Applied Therapeutics, Biostar family of funds, SpectraWave, Orchestra Biomed, Aria, Cardiac Success, MedFocus family of funds, and Valfix. Dr Sidhu has received research grants from the NHLBI during the conduct of the study; and has received personal fees from AstraZeneca and Sanofi-Regeneron. Dr. Hochman served as Principal Investigator for ISCHEMIA trial for which, in addition to support by NHLBI, devices and medications were provided by Abbott Vascular, Medtronic., St. Jude Medical, Volcano Corporation, Arbor Pharmaceuticals, AstraZeneca Pharmaceuticals, Merck Sharp & Dohme, and Omron Healthcare; and has received financial donations from Arbor Pharmaceuticals LLC and AstraZeneca Pharmaceuticals LP. Dr Bangalore has received research grants from the NHLBI during the conduct of the study; has received research grants from Abbott Vascular; and has received personal fees from Abbott Vascular, Biotronik, Pfizer, Amgen, and Reata.
Figures
Comment in
-
Treating Myocardial Ischemia Before Kidney Transplantation: Time for a Reappraisal.J Am Coll Cardiol. 2021 Jul 27;78(4):362-364. doi: 10.1016/j.jacc.2021.05.033. J Am Coll Cardiol. 2021. PMID: 34294271 No abstract available.
References
-
- Manske CL, Wang Y, Rector T, Wilson RF, White CW. Coronary revascularisation in insulin-dependent diabetic patients with chronic renal failure. Lancet 1992;340:998–1002. - PubMed
-
- Abbud-Filho M, Adams PL, Alberú J et al. A Report of the Lisbon Conference on the Care of the Kidney Transplant Recipient. Transplantation 2007;83:S1–S22. - PubMed
-
- Fleisher LA, Fleischmann KE, Auerbach AD et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;130:2215–45. - PubMed
-
- Arantes RL, Gowdak LH, Paula FJ et al. Myocardial scintigraphy and clinical stratification as predictors of events in renal transplant candidates. J Nephrol 2010;23:314–20. - PubMed
-
- Kahn MR, Fallahi A, Kim MC, Esquitin R, Robbins MJ. Coronary artery disease in a large renal transplant population: implications for management. Am J Transplant 2011;11:2665–74. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
