

Osteitis Fibrosa Cystica and pathological fractures-the classic but neglected skeletal manifestation of primary hyperparathyroidism: a case report
- PMID: 33990191
- PMCID: PMC8122575
- DOI: 10.1186/s12891-021-04326-1
Osteitis Fibrosa Cystica and pathological fractures-the classic but neglected skeletal manifestation of primary hyperparathyroidism: a case report
Abstract
Background: Osteitis fibrosa cystica is the classic manifestation of primary hyperparathyroidism (PHPT), occurs after prolonged exposure of bone to high serum parathyroid hormone (PTH) level. It has become increasingly rare due to early detection of PHPT.
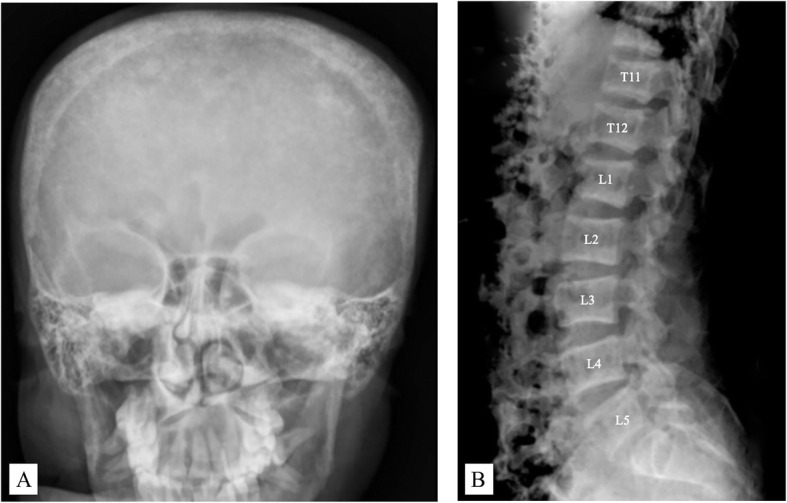
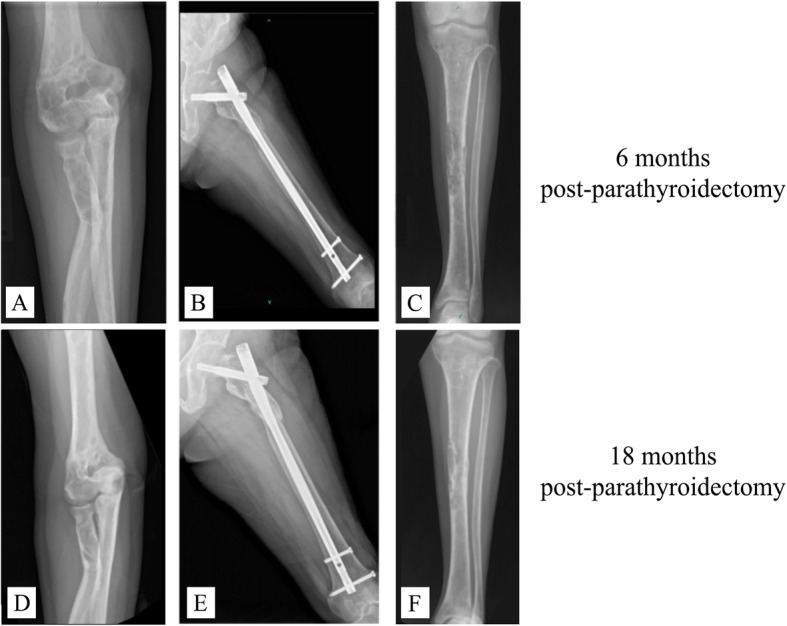
Case presentation: A 37-year-old woman was referred to our institution for fixation of multiple fractures of upper and lower extremities that had been reoccurring in the past 5 years. Her medical history showed right-shoulder, left-elbow, and right-femur fractures after a fall 5 years previously. One month ago, she sustained fractures of the right distal humerus, left tibia, and left femur without history of trauma. Upon arrival to our hospital, a thorough review of her plain radiographs demonstrated brown tumors at multiple sites, along with a salt-and-pepper appearance of the skull and a rugger-jersey spine, compatible with osteitis fibrosa cystica. Patient was diagnosed with PHPT, confirmed by high-corrected serum calcium (13.6 [8.6-10.0] mg/dl), low serum phosphate (2.2 [2.5-4.5] mg/dL), high serum alkaline phosphatase (1482 [35-105] U/L), and significantly elevated parathyroid hormone (PTH 3850 [15-65] pg/mL). A histologically confirmed, 2.5-cm parathyroid adenoma was removed by parathyroidectomy. Ten days later, closed reduction and internal fixation of the left proximal femoral shaft was performed. Pain and ambulation were significantly improved 6 months postoperatively. At the 1.5-year follow-up, fracture unions and complete mineralization of brown tumors were noted; the patient could ambulate with neither pain nor an assistive device.
Conclusions: PHPT has become more asymptomatic in countries where routine calcium screening is performed. Nevertheless, the classic skeletal involvement, osteitis fibrosa cystica, should not be overlooked, particularly in young patients who present with a low-energy fracture.
Keywords: Case report; Osteitis fibrosa cystica; Pathological fracture; Primary hyperparathyroidism; Skeletal manifestation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Panagopoulos A, Tatani I, Kourea HP, Kokkalis ZT, Panagopoulos K, Megas P. Osteolytic lesions (brown tumors) of primary hyperparathyroidism misdiagnosed as multifocal giant cell tumor of the distal ulna and radius: a case report. J Med Case Rep. 2018;12(1):176. doi: 10.1186/s13256-018-1723-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
